
記住我


Intraperitoneal chemotherapy, which was proposed approximately 30 years ago, has been extensively studied in both preclinical and clinical studies, and its usefulness has been demonstrated [5]. In 2005, the US National Cancer Institute (NCI) and Gynecologic Oncology Group conducted a meta-analysis of seven randomized controlled trials that had been completed until then, and found that intraperitoneal chemotherapy reduced the risk of death by 21.6% [7]. This important information was released as a clinical announcement from NCI in January 2006. This announcement indicated that intraperitoneal administration of cisplatin or cisplatin and paclitaxel should be considered for stage III epithelial ovarian cancer without residual tumor after radical treatment.
Despite this recommendation, IP chemotherapy has not been widely accepted in clinical practice [8]. There are several reasons for this avoidance of IP chemotherapy. First, there is uncertainty regarding IP chemotherapy efficacy related to trial design issues, such as imbalance in drug dosage and lack of comparison with standard chemotherapy. Second, there are concerns about cisplatin toxicity and peritoneal irritation caused by IP administration of paclitaxel. Third, there are concerns about the IP port which includes fear of port related complications and their subsequent management.
Several study groups initiated clinical trials, with the intention of addressing these issues with improved trial designs [9,10,11]. These include the GOG252 study conducted by GOG in the United States, the OV21/PETROC study, an international joint study conducted mainly in Canada and Europe, and the iPocc study, an international joint study conducted mainly in Japan.
1. Fig. 1
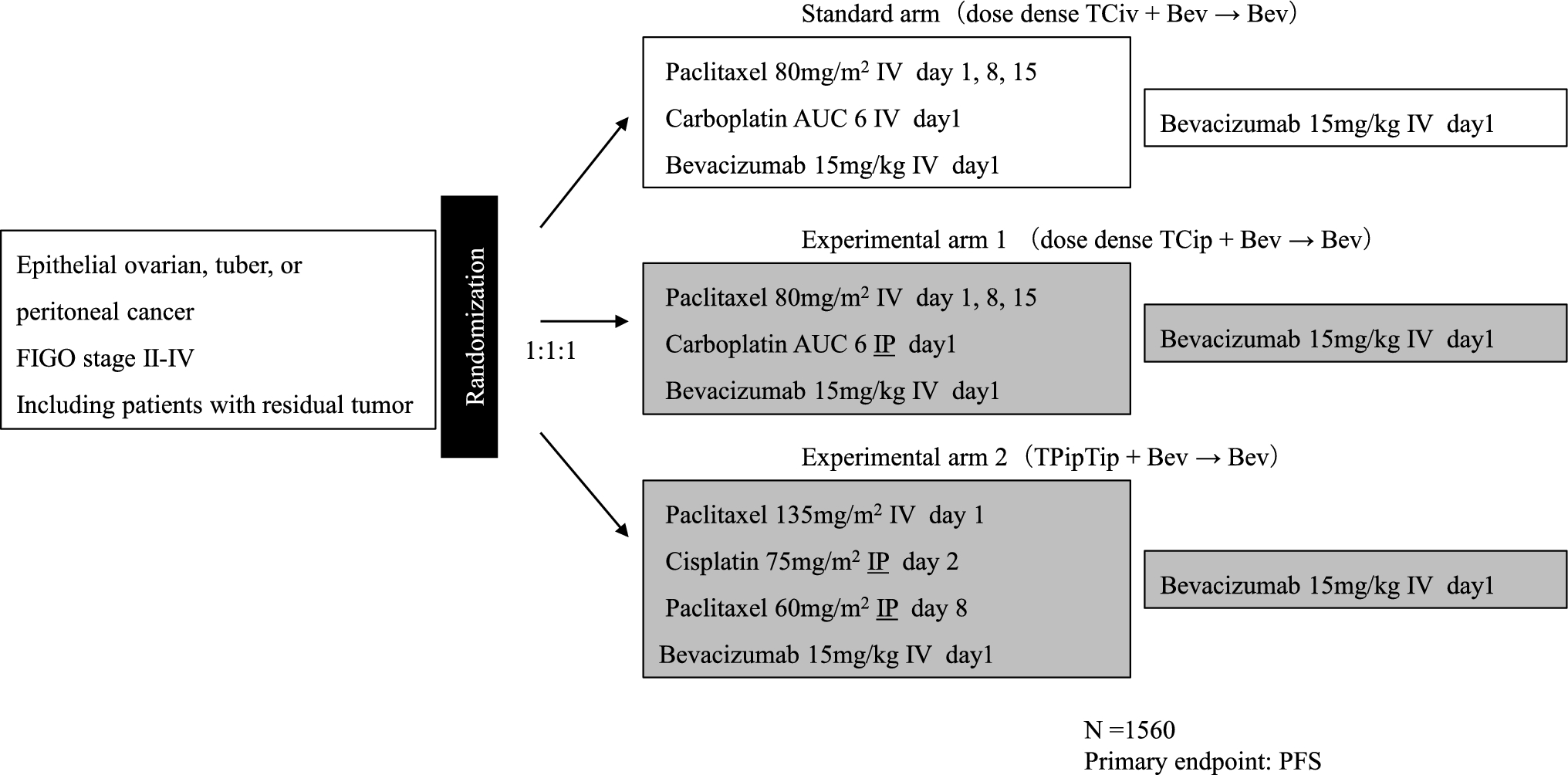
GOG252 study design. IV intravenous administration, IP intraperitoneal administration
The GOG252 study targeted women with primary treatment for epithelial ovarian cancer in FIGO stage II–III, including suboptimal cases with residual tumors of 1 cm or more in maximum diameter after primary cytoreductive surgery (PDS), and 1560 patients were enrolled. Bevacizumab was administered as concomitant and maintenance therapy in all arms. The median PFS for ddTCiv + Bev → Bev therapy, ddTCip + Bev → Bev therapy, and TPipTip + Bev → Bev therapy was 24.9 months, 27.4 months, and 26.2 months, respectively. The hazard ratios of ddTCip + Bev → Bev therapy and TPipTip + Bev → Bev therapy for ddTCiv + Bev → Bev therapy were 0.925 (95% CI 0.802–1.07) and 0.977 (95% CI 0.847–1.13), respectively, and there was no significant improvement in PFS. Similarly, no improvement in overall survival (OS) was observed.
2.OV21/PETROC study (Fig. 2) [10].
Fig. 2
OC21/PETROC study design. TC therapy: paclitaxel plus carboplatin combination therapy, IDS interval debulking surgery, IV intravenous administration, IP intraperitoneal administration. This study uses a pick-up the winner strategy. The winner arm in the phase II part will be compared to standard arm in the phase III part
The OC21/PETROC study targets women with FIGO stage III epithelial ovarian cancer who have received interval debulking surgery (IDS) after neoadjuvant chemotherapy (NAC) (3 to 4 cycles of TC therapy) to reduce residual tumor to less than 1 cm. This study was planned as a phase II/III study. First, TCip + Tip therapy and TPip + Tip therapy were compared in the phase II part; subsequently, the winner and the standard treatment are compared in the phase III part. TCip + Tip therapy, which was less toxic, was chosen as the winner arm in the phase II portion of the study, but could not complete the phase III study due to lack of funding. There was a trend toward less progression at 9 months with TCip + Tip therapy, 38.6 vs. 24.5% (P = 0.065). In addition, the hazard ratios for PFS and OS were 0.82 (95% CI 0.57–1.17, P = 0.27) and 0.80 (95% CI 0.47–1.35, P = 0.40), respectively, and no significant difference was observed due to insufficient power.
3. Fig. 3
iPocc study design. IV intravenous administration, IP intraperitoneal administration, NAC neoadjuvant chemotherapy, IDS interval debulking surgery
The iPocc trial purely compared ddTCiv therapy and ddTCip therapy among FIGO stage II to IV epithelial ovarian cancer, and all conditions other than the administration route of carboplatin are the same. Similar to the GOG252 study, it also included suboptimal patients after PDS and allowed IDS after 3 to 5 cycles of NAC. This study was based on two hypotheses: (1) carboplatin IP improves survival of patients with advanced epithelial ovarian cancer when combined with weekly intravenous paclitaxel 80 mg/m2 compared to intravenous carboplatin, and (2) IP therapy improves the prognosis of suboptimal patients after PDS. Median PFS was 20.7 months with ddTCiv therapy vs. 23.5 months with ddTCip therapy, hazard ratio 0.83 (95% CI 0.69–0.99, P = 0.041), and IP carboplatin significantly improved PFS, for more than 5-10 years. In subgroup analysis, ddTCip therapy tended to have a favorable prognosis regardless of residual tumor size, FIGO stage, age, and PS. The median OS was 67.0 months for ddTCiv therapy versus 64.9 months for ddTCip therapy, with a hazard ratio of 0.95 (95% CI 0.77–1.17, P = 0.41), and no improvement in prognosis was observed with IP carboplatin. All grade abdominal pain (34.7 vs. 51.7%), catheter infection (0.7 vs. 10.1%), and vaginal stump leakage (0.3 vs. 5.7%) were more common in ddTCip therapy, but there was no difference in the incidence of grade 3 or higher toxicity: 96.0 vs. 93.2%.
留言 (0)