This retrospective observational case series demonstrated that that age, BAD-D, and TBIv2 could predict ectasia progression in young patients with KC or suspected KC. According to a recent meta-analysis [5], young patients have a significantly increased risk for KC progression. Therefore, early detection and frequent follow-up for prompt initiation of appropriate interventions are necessary for these patients.
The biomechanical properties of the cornea have been studied, particularly for the detection of subclinical KC and ectatic corneal disease. However, little is known about long-term corneal biomechanical changes in unoperated eyes with KC. In our recent study that involved the evaluation of corneal biomechanical changes over three years, we found that in patients with very asymmetric ectasia, corneal softening may occur in the fellow eye having normal topography and not normal tomography [12]. Moreover, TBIv2 has been recently reported to enhance ectasia detection [7]. Based on these findings, we hypothesized that evaluating corneal biomechanical properties could facilitate the prediction of ectasia progression. Separating the KC group (including “forme fruste keratoconus” (FFKC)) from the “suspected KC” group (patients at risk but currently unaffected) would help draw clearer conclusions. However, in studying progressive diseases such as KC, with a high risk of progression in young individuals, focusing initially on young patients across all groups, as we did in this study, is clinically meaningful to determine “whether progression occurs.” Therefore, we included all groups in the present study. The results of the present study indicate that in young individuals, baseline TBIv2 may be a potentially useful prognostic marker of ectasia progression, whereas baseline BAD-D can be used for establishing a definitive diagnosis.
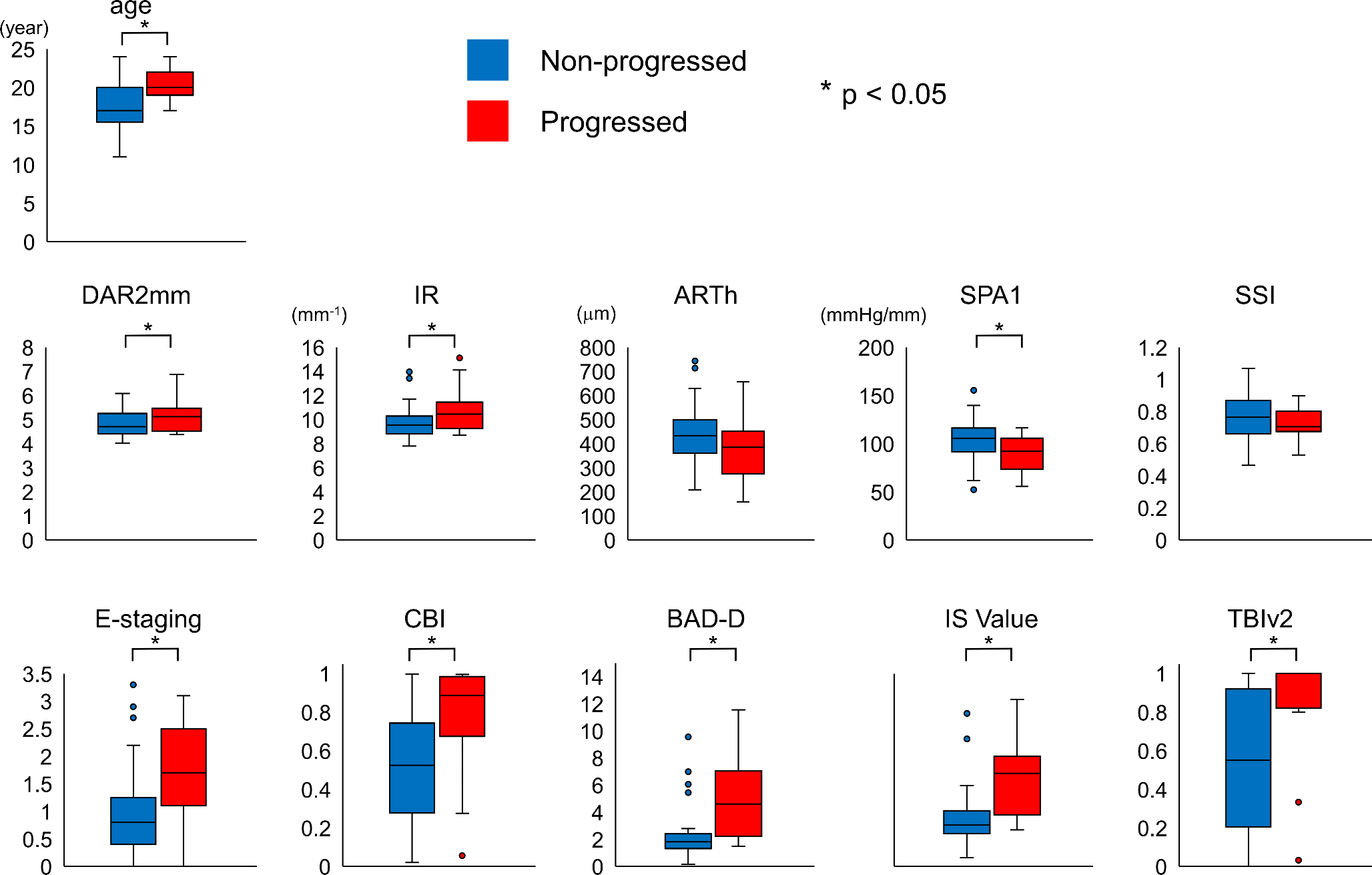
Previously, assessment of the progression of KC was based on clinical parameters [13,14,15]. Advanced corneal imaging techniques have improved screening, diagnosis, classification, and severity staging for clinical follow-up in cases of KC and ectatic corneal diseases [16, 17]. The progression of KC is now more commonly documented using corneal topography or corneal tomography [18,19,20,21,22,23]. However, little is known about the prognostic evaluation of the risk of progression. In the present study, BAD-D combined with age had high specificity (82%), whereas TBIv2 combined with age had high sensitivity (82%). BAD-D is useful for establishing a definitive diagnosis because of its high specificity in patients confirmed to have KC. Moreover, it may be useful in decision-making regarding the next treatment steps for patients confirmed to have KC. On the other hand, TBIv2 is highly sensitive, and although it is associated with a higher number of false positives than BAD-D, it is effective and can be used to confirm a negative test result. From this perspective, TBIv2 may be useful for predicting the progression of KC. Earlier awareness of the risk of ‘silent’ progression of KC would be helpful for detecting subtle progressive changes during clinical monitoring. A recent study with a one-year follow-up period, which was conducted using molecular biology testing, indicated that the level of interleukin-13 in combination with nerve growth factor in tears can predict the progression of KC [24]. The pathogenesis of KC is related to a combination of genetic, biomechanical, biochemical, and environmental risk factors, including inflammation [1,2,3, 25]. As multimodal imaging tools are fundamental for corneal assessments in patients with KC, multimodal prognostic evaluations, such as molecular biology testing and tomographic and biomechanical assessment, could be useful for predicting the progression of KC in the future. However, future studies with a large population of younger participants of different ethnicities are warranted to verify the predictive potential of these assessment methods for KC.
We enrolled eyes with KC of varying severities, ranging from very mild to advanced KC, and borderline cases of suspected KC in this study. We found that 58% of eyes with bilateral KC showed progression. This finding is comparable to that of a study conducted in Scotland [26], which indicated that 41% of young patients with KC (mean age 18, range 14–21) showed progression over a period of four years. In patients with very asymmetric ectasia and clinical signs of KC in one eye, the fellow eye with normal topography is referred to as FFKC. Although there is no unified definition of FFKC, the most widely used definition in various studies is “fellow eye of a clinical KC eye that has no clinical or topographic signs of KC” [27]. However, if the other ectatic eye has topographic KC signs without clinical signs, it cannot be termed ‘FFKC’. Notably, precise terminologies for describing these conditions are lacking. Considering that having “typical corneal topography” is included as a criterion in the revised Amsler–Krumeich classification [28], we specifically defined in the present study “the fellow eye with normal topography in a case of very asymmetric ectasia with the other eye showing clinical KC signs or at least topographic KC signs.” An improved classification system that considers the current diagnostic tools should be established.
In the present study, the patients with suspected KC showed no clinical or topographic KC signs bilaterally. The details of the optical characteristics of borderline KC are unknown. It is possible that some cases are close to “bilateral FFKC” [29]. Recently, we reported that patients with borderline suspected KC had significantly greater total higher-order aberrations and coma from the posterior corneal surface and whole eye than normal controls [30]. However, the heterogeneity of the study population is one of the limitations of the study. Some of the patients had severe astigmatism, whereas those who visited the hospital for a thorough examination because of a family history of KC did not necessarily have a high degree of astigmatism. The frequency of eye rubbing (76.9%) was higher in the young patients enrolled in this study than that (58.5%) from KC across all age group in our previous study [31]. Nevertheless, careful follow-up is recommended for these patients even if KC was initially excluded. In addition, a more extensive case series that includes a sub-analysis performed according to the type and amount of astigmatism would be interesting.
This study has some limitations. A retrospective study of young patients with KC or suspected KC who were followed for more than two years might be biased. Patients who subsequently had no complaints or were deemed non-progressive may not have been followed. The ABCD grading system alone would not be used to determine progression. However, it is useful to investigate the variation in clinical features of KC. Therefore, we used ABCD grading system in this study. Future studies using another classification systems should be considered. Some patients used soft or rigid gas-permeable contact lenses. However, owing to the retrospective nature of the study, the duration of contact lens discontinuation before examinations varied among patients. Ideally, patients should have discontinued contact lens use for a prolonged, standardized period before testing. However, it is often challenging for patients with KC to do so, as discontinuing lens wear could significantly impair their quality of life and vision. The current study was a single-center study with a small sample size. A follow-up multicenter study with a larger sample size would be ideal for characterizing the progression of ectasia in the Japanese population. Even though the patients in the suspected KC group were clinically suspected to have KC, the possibility of “eyes with corneal shape abnormalities that are not KC” could not be ruled out. Further longitudinal follow-up and multimodal assessments are essential for improving the predictive ability of the studied parameters for ectasia progression.
In conclusion, this study demonstrated that enhanced corneal biomechanical parameters may predict ectasia progression. Clinical follow-up of young patients with KC or suspected KC for more than two years showed that baseline BAD-D and TBIv2 have similar predictive values for ectasia progression but can be used differently. Baseline TBIv2 could aid the detection of ectasia susceptibility and identify patients with a risk for ectasia progression, mainly in cases of suspected but excluded KC if there are no abnormal topographical and clinical signs. Baseline objective tomographic analysis, such as that for deriving BAD-D, should still be considered for confirming the diagnosis.







留言 (0)