This systematic review and meta-analysis shows that nocturnal BP has an impact on retinal small vessels, although results may vary significantly according to the parameters under evaluation, either retinal (i.e., retinal arteriolar and venular widths, their ratio, or RVO) or ABPM-derived (dipping status, the degree of BP dipping, or absolute levels of 24-hour, daytime, or nighttime BP).More specifically, we conducted a meta-analysis demonstrating that categorization according to dipping status (i.e., dippers vs. non-dippers) is associated with altered retinal venular, yet not arteriolar, diameters. Furthermore, this systematic review provides some evidence that increased nighttime BP is associated with decreased retinal arteriolar width [16, 18], although these results were not unanimously reported [17]. However, due to divergent evaluated outcomes and different grouping of patients, we were not able to meta-analyze these data in order to quantitatively assess the impact of absolute levels of nighttime BP on retinal microvascular alterations. Finally, there is limited evidence that increased nighttime BP correlates with RVO [20], although it does not seem to affect the development of macular ischemia in patients with already established branch RVO [19].
Our finding that non-dippers exhibit increased values of CRVE is in line with a large body of evidence supporting that larger CVRE is associated with increased CVD risk and adverse CVD outcomes. In the Atherosclerosis Risk in Communities (ARIC) Study, wider retinal venules as well as narrower retinal arterioles conferred long-term risk of mortality and ischemic stroke in both sexes, and increased risk of coronary heart disease in the female population [22]. More recent analysis from the ARIC Study showed that CRVE widening was further associated with larger left ventricular size, higher prevalence of left ventricular hypertrophy, and worse measures of diastolic and systolic function over the mean 16-year follow-up period, and the same was observed for CRAE narrowing [23]. However, the most concrete evidence regarding the clinical significance of retinal venular dilatation comes from several population-based studies that show an association with the progression of cerebral small vessel disease, increased risk of lacunar stroke, ischemic and hemorrhagic stroke [22,23,24,25]. These data reinforce the hypothesis that the retinal microvasculature provides a direct “window” to the brain, further suggesting that increased CRVE may serve as an early marker of cerebral vascular disease.
Whereas venular width was associated with dipping status, the present meta-analysis does not support such an association with CRAE. Oppositely, our systematic review points towards an association of CRAE, yet not with CRVE, with absolute nighttime BP levels. These divergent findings should be considered as complementary, rather than contradictory, and imply a different prognostic role for each retinal microvascular diameter (arteriolar or venular). Epidemiological data indicate that non-dipping pattern confers a higher risk of future stroke [26, 27]. As mentioned above, retinal venular widening may be used as an early indicator of future risk of stroke. Taken together, it could be hypothesized based on our results that the non-dipping pattern provokes cerebral vascular injury, that can be non-invasively assessed through the study of retinal venular width at pre-symptomatic stages.
On the other hand, there is an inherent relationship between absolute levels of BP and retinal arteriolar diameters. Elevated levels of both conventional and 24h ambulatory BP primarily affect the retinal arterioles, especially during early stages of hypertension, and have been associated with decreased retinal arteriolar width [28]; our study further reinforces this evidence by suggesting an inverse association between CRAE and nighttime BP levels as well [16, 18]. This association was not reproduced in a study that dichotomized nighttime systolic BP according to the conventional cut-off threshold of 120 mmHg [17]; therefore, we were not able to meta-analyze these studies. Remarkably, the association between retinal arteriolar width and BP is bi-directional. The strong impact of elevated BP on the retinal arterioles has long been known and characterizes the first stage of hypertensive retinopathy according to the Keith-Wagener classification. [2] Vice versa, retinal arteriolar narrowing may predict future onset of hypertension to a larger extent than retinal venular width, and supports the concept that generalized microvascular remodeling, as observed in the retinal microvasculature, precedes the onset and progression of hypertension [29].
Regardless of the causality of the observed associations, our study provides some important clinical implications. 24h ABPM is being increasingly recognized as the method of choice, whenever possible, for establishing the diagnosis of hypertension and for subsequent BP monitoring [30]. BP recording throughout the whole 24h period offers the unique advantage of diagnosing nocturnal hypertension and identification of dipping status. Based on the results of the present study, identification of elevated nighttime BP levels as well as non-dipping profile warrants a thorough screening for pre-symptomatic injury in divergent vascular beds, including the retinal microvasculature. Vice versa, phycisians should be alert upon identification of subtle microvascular alterations in the retinal microvasculature that may imply altered day-to-night BP variation, and consider implementation of 24h ABPM. Finally, the results of our study generate further hypotheses regarding the potential effects of chronotherapy, i.e., treatment aiming at restoring the nocturnalcircadian BP rhythm, on the reversal of microvascular injury related to elevated nighttime BP.
Limitations of the present study that downgrade the certainty of the provided evidence are inherent to the limitations of the included studies, which were in their majority observational, non-randomized and applied different entry criteria and outcome measures. Further limitation of the study is that the included studied use different methodology to assess retinal vasculature. Hence, owing to the heterogeneity of outcomes and the different synthesis of study populations, it was not feasible to meta-analyze data regarding the association between CRAE and nighttime BP. We were able to perform a meta-analysis of three available studies regarding the association between dipping status and retinal microvascular diameters; however, one of these studies was conducted in a distinct population of normotensive patients with type 1 diabetes mellitus [18]. Although this does not negate the impact of dipping status on the retinal microvasculature, it further highlights the need for appropriately designed studies to evaluate the association between nocturnal BP and retinal microvascular alterations.
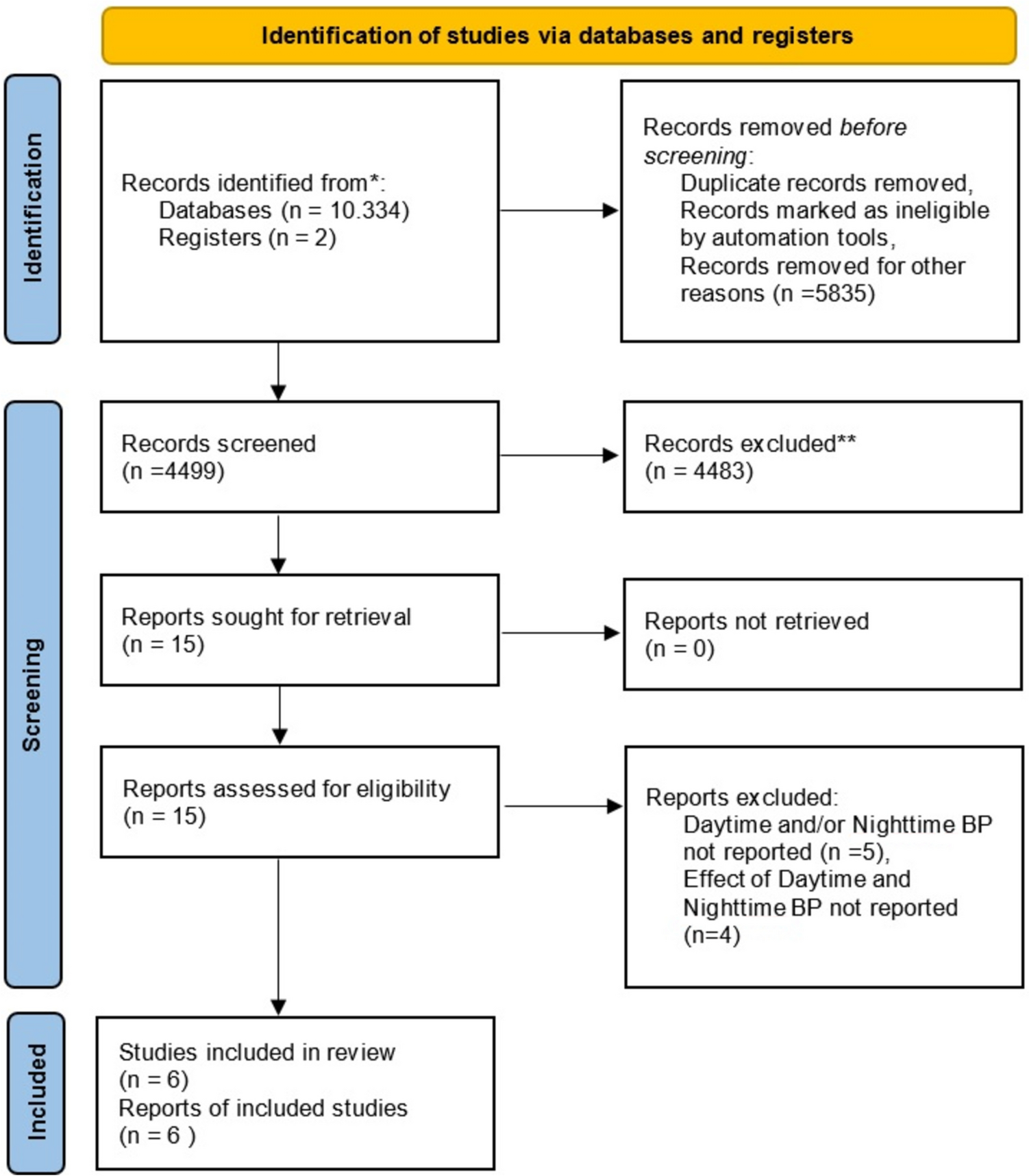
In summary, this is the first effort to summarize evidence on the effects of day-to-night variation of BP on the retinal small vessels. According to the findings of the present systematic review and meta-analysis, non-dipping status may be associated with retinal venular dilatation, and elevated nighttime BP with retinal arteriolar narrowing. Further studies are warranted to elucidate the impact of nocturnal BP patterns in the retinal microvasculature. However, these results underscore the clinical significance of nocturnal BP as a mediator of generalized vascular impairment, and call for a more careful evaluation of patients who present with abnormal nighttime BP in the context of subclinical vascular injury.






留言 (0)