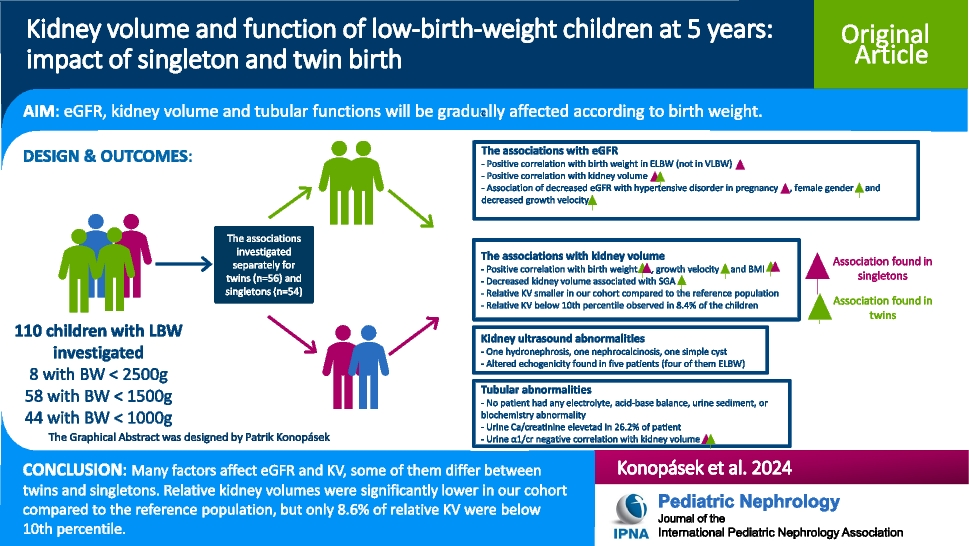
We report a comprehensive study exploring the associations between LBW, numerous prenatal, perinatal and postnatal factors, and various kidney parameters in 2 distinct populations: singletons and twins. It has been more than 30 years since Brenner et al. proposed the hypothesis that decreased glomerular count leads to hyperfiltration and glomerular hypertension due to decreased filtration surface area with subsequent glomerular sclerosis [2, 5, 28]. Numerous studies have aimed to investigate eGFR and KV in children and adolescents born with LBW [10,11,12,13,14,15,16,17,18,19]. In the study of Japanese adolescents, eGFR was found to be positively correlated with BW. LBW individuals and those who were overweight had higher odds for CKD stage 2 [10]. A few studies on 11-year-old children found significantly lower eGFR in ELBW individuals compared to the control group; in one study, those born SGA had even lower eGFR [11,12,13]. In two studies on young adolescents aged 12–15 years, those born with a LBW had lower eGFR than those born with normal BW, and eGFR was even lower in VLBW individuals [14, 15]. In a Polish longitudinal study, ELBW born children had significantly higher CyC and lower KV compared to the control group at age of 7 and 11 years [9]. Nine-year-old Bangladeshi LBW children were found to have lower eGFR compared to normal BW controls and lower KV at age 4.5 years than normal BW controls [16]. A study of 6–7-year-old children found a significantly lower KV in ELBW children compared to controls [17]. In the study of preschool children aged 5.7 ± 1.4 years, ELBW had significantly lower KV than VLBW children, but eGFR did not differ between the groups [18]. Young adults born at gestational age < 32 weeks were found to have significantly reduced KV, and renal structural anomalies were present in 8 of 51 individuals (nephrocalcinosis, pyelocaliceal dilatation, uretero-pelvic junction obstruction, ureter dilatation, extrarenal pelvis, and ureter duplication and ureterocele) [19].
In our study, we found a positive correlation between BW and eGFR in ELBW children, while in those born with BW ≥ 1000 g, eGFR remained constant. The explanation could be that in those born with BW ≥ 1000 g, the remaining nephrons are still able to maintain normal eGFR, while in ELBW children, the pool of nephrons is too small to maintain normal eGFR. KV showed positive correlation with eGFR in the whole cohort; the KV therefore seems to reflect indirectly the absolute pool of nephrons in 5-year-old children, but our results cannot be extrapolated to all populations. Based on the meta-analysis in adults from 2013, kidney size is not a suitable marker of nephron pool in adults [29]. We also found other factors associated with decreased eGFR, which were different in singletons (hypertensive disorders during pregnancy, AKI) and twins (decreased growth velocity, female gender). Based on the multivariable models excluding KV, BW and gestational age were associated with eGFR in singletons, while male gender, BW, growth velocity, and coffee drinking during pregnancy were associated with eGFR in twins. However, in models that included kidney volume, BW, gestational age, and growth velocity were no longer significant. These results indicate that KV appears to be a better predictor of eGFR than BW and gestational age at 5 years of age. In general, the results of our study support previous publications and show that many factors may have a significant impact on kidney health in LBW individuals. The association between LBW and CKD is very complex, with many variables that may influence the outcome.
The measurement of GFR has many significant limitations for routine practice; for that reason, an estimation using endogenous markers is the first-line examination. Creatinine is the most frequent marker used for GFR estimation. However, its use is limited by many non-GFR determinants. CyC seems to be less influenced by these determinants, but its use is limited by the price [30]. Designing a universal equation to precisely estimate GFR is one of the most challenging tasks in pediatric and adult nephrology. Many equations have been created for different populations, with combined creatinine and CyC equations showing the best performance [30]. We decided to use the creatinine-CyC-based CKiD equation; however, we found no study comparing different equations for eGFR with measured GFR in the LBW population. Therefore, we believe that the most appropriate equation for this specific population is unknown. This statement is supported by different equations used within the studies [9,10,11,12,13,14,15,16,17,18].
We describe a positive correlation between BW, BMI, growth velocity and KV. SGA was associated with lower KV in twins. Total KV was in general better associated with all the factors than rKV. Based on our multivariable analyses, both BW and BW relative to gestational age were associated with KV. Specifically, when comparing children with the same BW, those with a lower BW percentile for their gestational age had lower KV compared to those with lower gestational age but higher BW percentiles. The same pattern was observed for eGFR. Both BW and growth parameters were already demonstrated to correlate with KV, as previously mentioned [9, 16, 17, 31]. Relative kidney volumes of both kidneys in our cohort were significantly lower than those of the reference population reported by Scholbach et al. [26]. This result is not surprising, as many authors have found lower rKV in children and young adults with LBW compared to those with normal BW [9, 16, 19, 32]. However, only 10.5% of right rKVs, 3.8% of left rKVs, and 8.6% of the rKV for both kidneys in our study fell below 10th percentile according to the reference population [26]. This indicates that, despite the lower rKVs in LBW individuals, oligonephropathy is not more prevalent in this population. Sanderson et al. [33] found no significant difference in rKV in their cohort of ELBW adolescents compared to the same reference population [26]. However, their cohort consisted of only 42 children which likely contributed to the lack of statistical significance. In the same study, they reported that 14.3% of children had rKV below the 10th percentile. The higher percentage compared to our study could be explained by the lower mean BW in their cohort compared to ours (770.0 ± 173.1 g vs. 1109.7 ± 315.4 g).
Coffee consumption during pregnancy appeared to be a protective factor for both eGFR and KV. There are studies suggesting the protective effect of caffeine on neonatal AKI [34]. However, when interviewing parents, we were specifically interested in coffee consumption and therefore could have missed other beverages containing caffeine. Additionally, recall bias could have occurred as we inquired about information from 5–6 years ago. For these reasons, our results are not conclusive. We suggest that a study designed specifically to investigate the impact of caffeine intake during pregnancy on offspring kidney outcomes should be conducted.
There were only three ultrasound abnormalities (one hydronephrosis, one nephrocalcinosis, one simple cyst), and altered echogenicity was found in five patients. In a previous study, nephrocalcinosis was prevalent in infants born with LBW with especially high prevalence in those born ELBW [35]. In our cohort, only one patient had nephrocalcinosis. Our study suggests potential spontaneous resolution of nephrocalcinosis during childhood without specific consequences for the population, although this is only our assumption, as we do not know the prevalence of nephrocalcinosis in early childhood in our cohort. From those patients with altered echogenicity, four were born with ELBW, one of them has already been published as a case report (the patient with BW of 370 g) [27]. We believe the altered echogenicity is the result of abnormal kidney development due to LBW, as we did not identify another explanation for this, such as cystic kidney disease or glomerulonephritis. Our hypothesis is supported by the altered echogenicity being found mainly in ELBW children who are expected to have the worst kidney outcomes.
We found an elevated U-ca/cr in 26.2% of our patients, which is similar to a previous report [36]. We also found a negative correlation between U-α1/cr and KV, and small correlation with eGFR almost reached significance. Matsumura et al. [36] described a high prevalence of tubular dysfunction (the definition based on urine abnormalities) in ELBW individuals. During follow-up, some parameters improved while others remained stable or even got worse [36]. Zaffanello et al. [18] found higher excretion of α1-microglobulin in ELBW compared to VLBW children. The real significance of these urine abnormalities for the patients is questionable. In our study, no patient had either any electrolyte, acid–base balance, urine sediment or biochemistry abnormality, and only one child was found to have nephrocalcinosis. As there was a negative correlation between U-α1/cr and KV, the U-α1/cr may be a possible indirect marker of a quality of kidney development, but KV by itself gives us a lot of information and is easily estimated by kidney ultrasound, which is a cheap and readily available examination. Further investigation will show whether urine tubular abnormalities in LBW individuals may have a real clinical impact on patients’ health and diagnostic approach.
The strength of our study is its complexity. We investigated the association between a significant number of exposures and various kidney parameters. Most of the exposures were obtained directly from hospital documentation, minimizing the risk for bias during collection. We used creatinine-CyC-based equation, which is considered to provide the best performance. Additionally, our cohort included a significant number of twins, allowing us to study two different populations within the same study protocol, and we provided data on twins, which are scarce.
Our study has some limitations. We had to separate our cohort into two smaller groups due to the high proportion of twins in our cohort. However, studies on twins bring valuable information about individuals with similar environments and genetic predispositions. Also, there might be a selection bias in our study. However, children in our cohort had very similar distributions of birth parameters compared to excluded patients; we therefore believe that our cohort represents the standard distribution in the population. We were only able to investigate correlations and associations within our cohort, as there was no control group in the study. This was a cross-sectional study which does not allow us to describe changes of investigated parameters during a time period. We studied the potential effect of coffee drinking during pregnancy; however, there was a high probability of confounding and recall bias. Therefore, even though our results were significant, they are inconclusive. We found that rKV of both kidneys were lower in our cohort compared to normative data. However, we used the kidney volumes from the whole cohort mixing singletons and twins together.
In conclusion, in our study on 5-year-old LBW children, we found many factors to be associated with eGFR and KV in this population. Some of these factors differed between twins and singletons, which shows how many variables may have a significant impact on kidney health in these individuals. Patients born with a BW ≥ 1000 g are still able to maintain normal eGFR, while eGFR in ELBW patients significantly decreases with decreased BW. Importantly, eGFR seems to be better predicted by KV than by BW and gestational age in LBW children based on the multivariable models. BW and growth parameters correlated with KV, and tKV is in general better associated with all investigated parameters than rKV. Relative kidney volumes were significantly lower for both kidneys compared to the reference population; however, we did not find a higher prevalence of oligonephropathy in our cohort. LBW individuals, especially those born ELBW, may have altered kidney echogenicity likely as a sign of abnormal kidney development associated with LBW. Tubular dysfunctions in LBW individuals have questionable impact in clinical practice, as no laboratory signs such as electrolyte, acid–base balance, urine sediment or biochemistry abnormalities were found in our study.





留言 (0)