
記住我
Breech presentation is the most common form of malpresentation, accounting for 3%–4% of all deliveries at term (1). Persistent breech presentation may be associated with abnormalities of the baby, the amniotic fluid volume, the placental localization, or the uterus. It may be due to an otherwise insignificant factor, such as corneal placental position, or it may be due to chance (2). Many breech births’ resulted in very high perinatal mortality and morbidity due to a combination of trauma, birth asphyxia, prematurity, and malformation. One study in Ethiopia reported that 19.4% of neonates undergoing term breech deliveries have long-term morbidity up to school age, irrespective of the mode of delivery (3).
A wide range of management policies have been instituted to reduce perinatal morbidity and mortality. On the other hand, the breech presentation delivery approach is a controversial issue in obstetrics. How to cope with breech delivery (vaginal or C-section) has been discussed to find the safest in terms of morbidity (4). However, a planned caesarean section is better than a planned vaginal birth for the term fetus in the breech presentation (5, 6). The Term Breech Trial study revealed that perinatal mortality or serious neonatal morbidity was significantly lower for the planned caesarean section group than for the planned vaginal birth group (7).
The American College of Obstetricians and Gynecologists recommends that cesarean delivery be offered to women with a breech presentation if certain criteria are met, such as if the estimated fetal weight is greater than 3,500 g, if the mother has a contracted pelvis or other factors that may make vaginal delivery difficult, or if the baby is in an incomplete breech presentation (i.e., one or both feet are below the baby's buttocks) (8). Cesarean delivery may also be recommended if the baby has a known medical condition that may make vaginal delivery risky. It is important to discuss the risks and benefits of both vaginal and cesarean delivery with your healthcare provider to make an informed decision. Cesarean deliveries are usually performed to reduce the risks to the infant, such as when the fetus is in a breech position rather than headfirst in the birth canal (9). But the risks to the mother caused by the surgical procedure may be greater than with a normal vaginal delivery (10).
The benefits of cesarean section breech delivery include a lower risk of injury to the baby during delivery, a reduced risk of oxygen deprivation, and a lower risk of incontinence and sexual dysfunction after the birth of the baby (11, 6). However, this procedure also carries some risks, such as a higher risk of bleeding, infection, and complications with anesthesia (12). In comparison to vaginal delivery, cesarean-section breech delivery may have a longer recovery time for the mother and may increase the risk of future pregnancies requiring cesarean delivery. Additionally, vaginal delivery is associated with a lower risk of complications such as bleeding, infection, and blood clots (13).
The World Health Organization (WHO) declared that the cesarean section rate should not exceed 10%–15%. However, unnecessary C-sections may be associated with an increased risk of maternal and neonatal mortality (14, 15). Studies done in Ethiopia show that a wide range of rates of cesarean sections among breech deliveries have been measured in several regions. Of all studies, more than half (6) were conducted in the Oromia region (16–20), one study in Harari (16), one study in Amhara (17), one study in the southern nation and nationality region (18), and one study in Addis Ababa (19). A total of 57,236 mothers who gave breech deliveries at the health institution were included in this systematic review and meta-analysis. A summary of the main characteristics of the papers included in this systematic review and meta-analysis. Despite several studies on the rate of cesarean section among breech deliveries, no systematic meta-analysis or meta-regression studies on the Ethiopian scale have been performed. Hence, the current study was devoted to performing a systematic review, meta-analysis, and meta-regression regarding the rate of cesarean section among breech deliveries in Ethiopia.
2 Methods 2.1 Protocol and registrationThis review was conducted to identify the prevalence of perinatal outcomes among breech delivery women in Ethiopia accordance to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guideline (Supplementary Material S2).
2.2 Eligibility criteriaStudies that scrutinized the rate of cesarean sections in breech delivery among women in Ethiopia were included. The study included all observational studies that had either the primary or secondary outcomes of the review. The pre-specified criteria for inclusion were: Population: delivered women or postpartum women; study area: only studies conducted in Ethiopia; publication condition: both published and unpublished research; study design: all observational study designs; and language: studies reported in the English language were included. Finally, all full-text papers published up until August 13, 2023, were included. This review excluded case series or reports, reviews, commentaries, and editorials.
2.3 Information sourcesThe articles were searched and retrieved from valid and reliable databases and website platforms such as the Web of Sciences, MEDLINE, EMBASE, SCOPUS, PubMed, and Google Scholar. We also tried to access different universities’ institutional repository sites found in Ethiopia. A direct Google search was also performed.
2.4 Search strategyThe search was accomplished using Medical Subject Headings (MeSH) and keywords with a combination of Boolean logic operators (AND, OR, NOT). The search strategy for advanced PubMed includes “cesarean section” [MeSH Terms] AND ((“breech”[All Fields] OR “breeches”[All Fields]) AND (“deliveries”[All Fields] OR “delivery, obstetric”[MeSH Terms] OR (“delivery”[All Fields] AND “obstetric”[All Fields]) OR “obstetric delivery”[All Fields] OR “delivery”[All Fields])) AND “ethiopia”[MeSH Terms]. The search strategies are presented in Supplementary Material S1.
2.5 Study selectionThe database search results were consolidated, and duplicate articles were manually removed using the reference management application (Endnote version X8). The titles and abstracts of the papers were then carefully evaluated. Three writers (IM, LDR, and AE) independently reviewed the full texts of the remaining publications to determine their eligibility based on predetermined inclusion and exclusion criteria. The objectives, methodology, population, and significant findings (rate of cesarean section among breech deliveries in Ethiopia and prevalence of breech delivery) of the full-text studies in English were then reviewed further. The two authors came to a logical agreement to handle any questions that developed during the extraction process, and the final agreement was finalized with the assistance of the authors (AD and IM).
2.6 Data extractionThe two authors (IM and AE) extracted the data independently using a Microsoft Excel 2016 sheet after identifying articles that meet the inclusion criteria. Different variables of interest were considered in the extraction and presented in the table of contents. The accuracy of the data extraction was checked by comparing the results produced by the two authors. The information used for meta-analysis from the included articles was extracted, which included the total number of breech deliveries (N), frequency of the occurrence of cesarean sections (n), measure of associations with a 95% CI, and effect size.
2.7 Data itemThe primary outcome of this meta-analysis is the rate of cesarean section among breech deliveries in Ethiopia. Breech delivery is the delivery of a fetus with a breech presentation. The secondary outcome of interest was the prevalence of breech deliveries. It is the proportion of breech deliveries among total deliveries in health institutions in Ethiopia.
2.8 The methodological quality of the studiesThe risk of bias was assessed using the Newcastle-Ottawa scale, which is a validated tool for assessing the quality of non-randomized studies (cross-sectional studies) (20). The risk of bias assessment tool includes the following domains: selection domain, including representativeness of the sample, non-respondents, and ascertainment of the exposure (risk factor); comparability domain (the subjects in different outcome groups are comparable based on the study design or analysis, and confounding factors are controlled); and outcome domain, such as assessment of the outcome and statistical tests. The included studies’ methodological validity and the quality of their conclusions were scrutinized. Two authors (AD and IM) assessed and scored the quality of the study using NOS. The mean score of the authors was utilized to make the final decision. Based on their performance against each tool indicator, the included studies were categorized as high, moderate, or low quality. Good quality is defined as 80% or more, moderate quality as 60%–80%, and low quality as below 60%. The quality score of the eleven studies ranges from 6 to 9, with most studies (8 studies) scoring eight. All eleven studies were considered of adequate quality for inclusion in the analyses.
2.9 Statistical analysisStatistical analysis was conducted using STATA 18 software. The meta-analysis data demonstrating adverse perinatal outcomes in breech deliveries among women in Ethiopia were presented using forest plots. A meta-analysis of the prevalence of adverse perinatal outcomes was done using a random effect model using the Der Simonian Liard method of analysis to reduce the heterogeneity of the included studies. Subgroup analyses were also performed based on several research parameters. Both bivariate and multivariate meta-regressions were performed to determine and identify the source of heterogeneity. A meta-analysis of observational studies was undertaken based on the recommendations of the I2 statistic given by Higgins et al. (an I2 of 75/100% and above implies considerable heterogeneity). To look for potential publication bias, the researchers utilized Egger's regression test, trim fill analysis, and a visual evaluation of a funnel plot. Sensitivity analysis was done using the leave-one-out meta-analysis method to identify the effect of a single study on the overall estimate and to identify the outliers.
3 Results 3.1 Search findings and risk of bias assessmentA total of 138 published and unpublished articles were found in databases and institutional repositories. Using Endnote and visual inspection, 31 publications were removed from all identified studies due to duplication. The remaining 107 studies were then maintained and screened based on title and abstract. After being vetted based on titles and abstracts, 89 were eliminated. Eighteen articles were considered eligible, and eight studies were removed because they assessed non-breech deliveries or were done outside Ethiopia. Finally, the systematic review and meta-analysis comprised 11 published and unpublished observational studies that met the inclusion criteria (Figure 1). A detailed review of the included research across eight domains yielded high-quality scores. Fortunately, all articles were included.
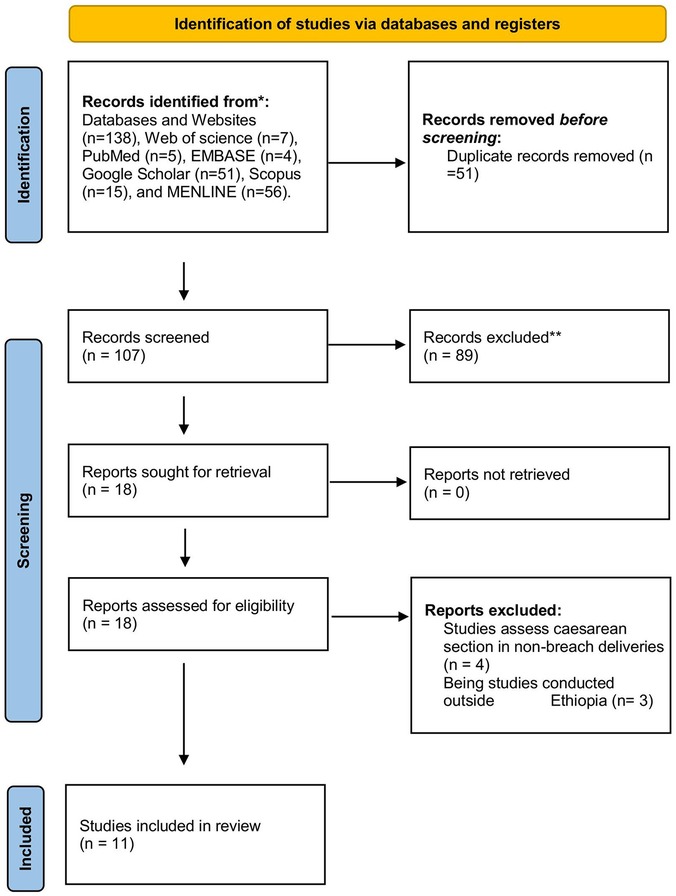
Figure 1. Flow chart showing the procedure of selecting studies for systematic reviews and meta-analysis up to 13/25/2023 G.C.
3.2 Characteristics of included studiesThis systematic review and meta-analysis comprised eleven observational studies (10 cross-sectional and one case-control study) that assessed the prevalence of breech deliveries and the rate of cesarean section among breech deliveries in Ethiopia. The sample size of the included studies ranges from a minimum of 612 in a study by Wadajo AT (21) to a maximum of 11,546 in studies done by Fentahun et al. (22). The included articles were published between 1995 (23) and 2022 (24). Of all the studies, more than half (6) were conducted in the Oromia region (16–20), one study in Harari (16), one study in Amhara (17), one study in the southern nation and nationality region (18), and one study in Addis Ababa (19). A total of 57,236 mothers who gave breech deliveries at the health institution were included in this systematic review and meta-analysis. A summary of the main characteristics of the papers included in this systematic review and meta-analysis (Table 1).
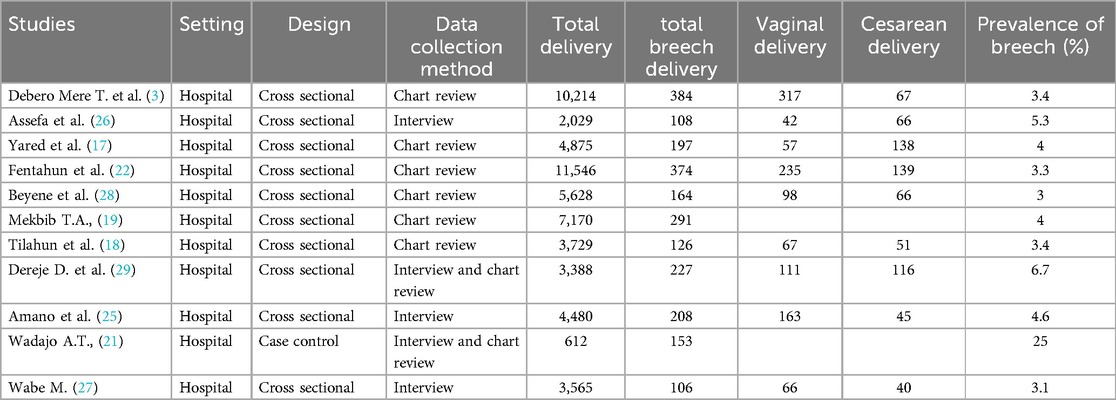
Table 1. Characteristics of included studies in this systematic review and meta-analysis in 2023.
3.3 Meta-analysis of the prevalence of breech deliveriesIn this meta-analysis, a total of 11 studies were considered. The prevalence of breech delivery ranges from 3% (95% CI: 2–3) to a maximum of 25% (95% CI: 22–29). The pooled prevalence of breech deliveries among women in Ethiopia was 5% [95% CI: 4, 6]. There is significant heterogeneity among individual studies (I2 = 97.32%) (Figure 2).
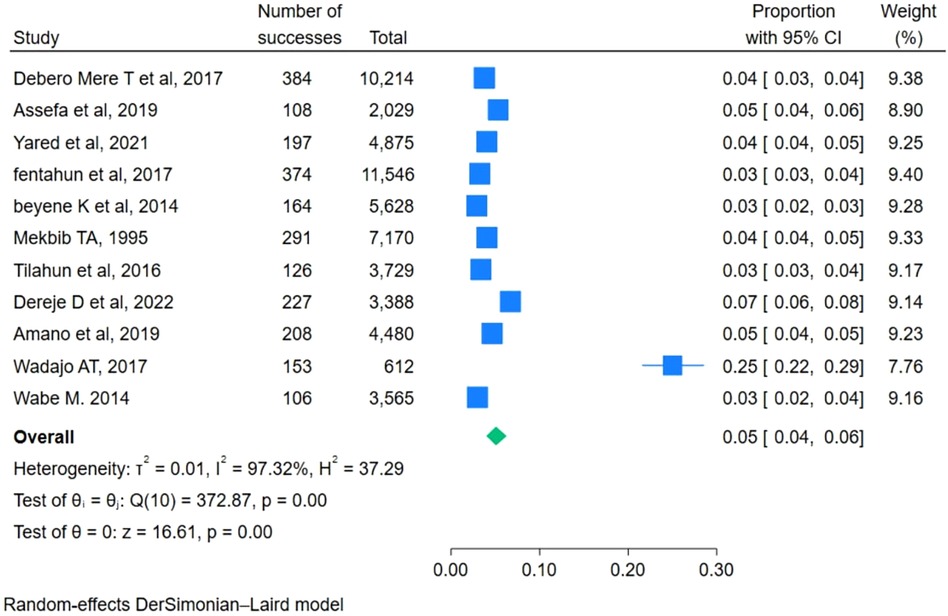
Figure 2. Pooled prevalence of breech deliveries among women in Ethiopica, 2023.
3.4 Subgroup analysis of prevalence of breech deliveriesBased on subgroup analysis by publication year, the highest prevalence of breech deliveries among women in Ethiopia was observed among studies conducted after 2014, which was 6% (95% CI: 4–8). The heterogeneity among the subgroups was different, and there was a decline in heterogeneity in studies conducted during and before 2014. Based on subgroup analysis by region, the prevalence of breech deliveries among women in Ethiopia was observed among studies conducted in the Oromia region at 7% (95% CI: 6–8) (Figure 3).
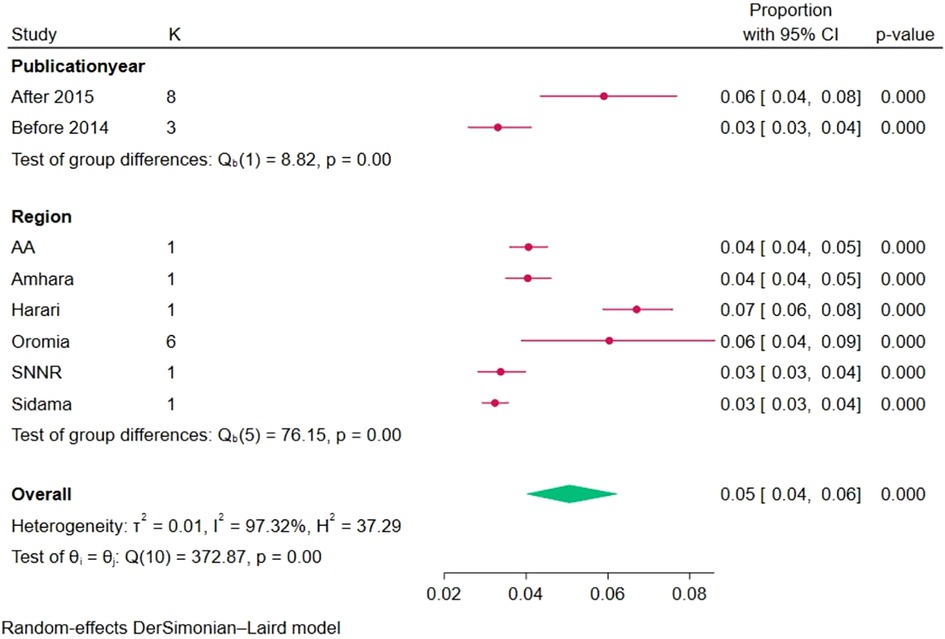
Figure 3. Subgroup analysis of the pooled prevalence of breech deliveries in Ethiopia based on region and publication year, 2023.
3.5 Publication biasTo observe publication bias, a visual inspection of the funnel plot was carried out, and it shows that there was no publication bias observed despite significant heterogeneity among studies (Figure 4). Egger's test shows that there was no small study effect on the estimate (P = 0.87). Furthermore, trim fill analysis also showed no difference in observed or combinations of observed and imputed effect size estimates in the random effect model utilizing Der Simonian Liard.
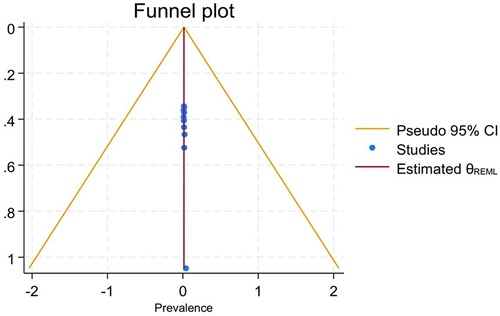
Figure 4. Funnel plot of the pooled prevalence of breech deliveries in Ethiopia, 2023.
3.6 Multivariate meta-regressionThe pooled prevalence of breech deliveries among women in Ethiopia shows that there was heterogeneity and the I-square test statistics were significant; a meta-regression analysis was performed (I2 = 97.32, P value = 0.001). Both bivariate and multivariate meta-regressions were conducted using different variables. The meta-regression study discovered that sample size was the source of the heterogeneity. However, other study-level covariates were not statistically significant (Table 2).
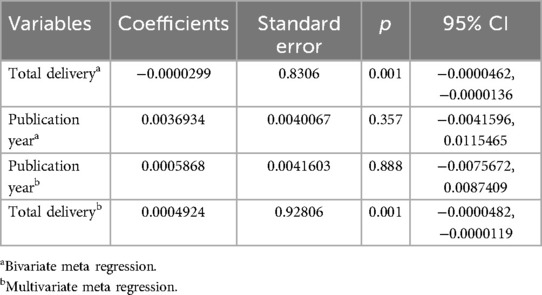
Table 2. Bivariate and multivariate meta-regression analysis to check heterogeneity, 2023.
3.7 meta-analysis of the rate of cesarean section among breech deliveriesOf the eleven studies, nine report the rate of cesarean section among breech deliveries in Ethiopia (3, 17, 22, 25–29). Of them, the rate of cesarean section ranges from 17% (95% CI: 14–21) to 70% (95% CI: 63–76). The overall pooled cesarean sections rate among breech deliveries in Ethiopia was 41% (95% CI: 29–54) (Figure 5).
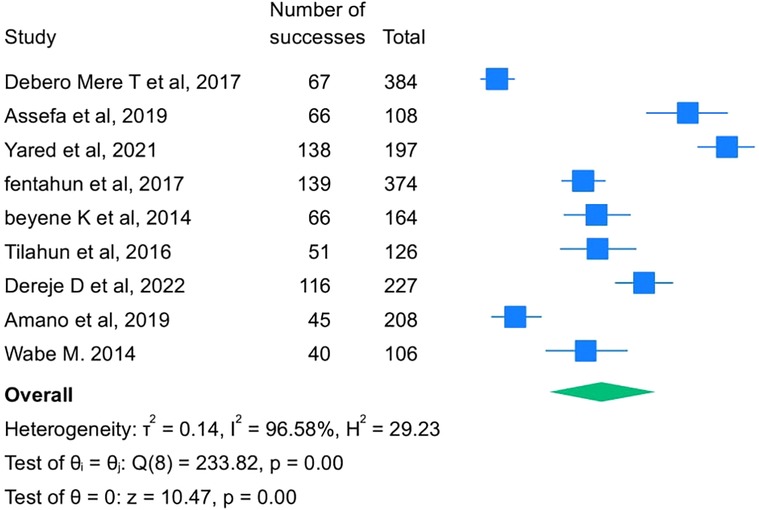
Figure 5. Rate of cesarean section among breech delivery among women in Ethiopica, 2023.
3.8 Subgroup analysis of the rate of cesarean section among breech deliveryBased on subgroup analysis by publication year, the highest rate of cesarean section in breech deliveries among women in Ethiopia was observed among studies conducted during and before 2014, which was 61% (95% CI: 55–67). Based on subgroup analysis by region, the highest rate of cesarean section in breech deliveries among women in Ethiopia was observed among studies conducted in the Oromia region, which was 65% (95% CI: 50–80) (Figure 6).
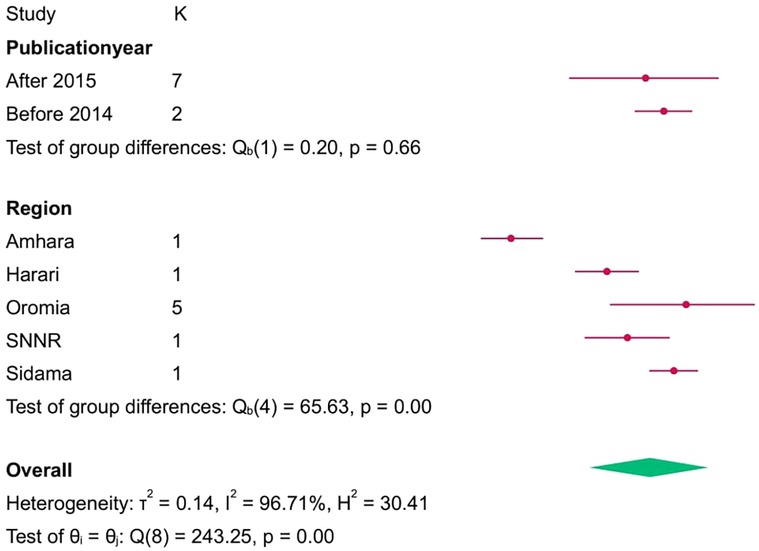
Figure 6. Subgroup analyis of the rate of cesarean section among breech delivery among women in ethipia, 2023.
3.9 Sensitivity analysisLeave one out of a meta-analysis. The Der Simonian Liard method was used to assess the effect of a single study on the overall estimate of the rest of the studies in the meta-analysis results and to identify outliers. As shown in the figure below, when individual studies were removed and the overall prevalence re-estimated, there was no such significant deviation from the previously determined prevalence (Figure 7). Furthermore, there were no outliers observed.
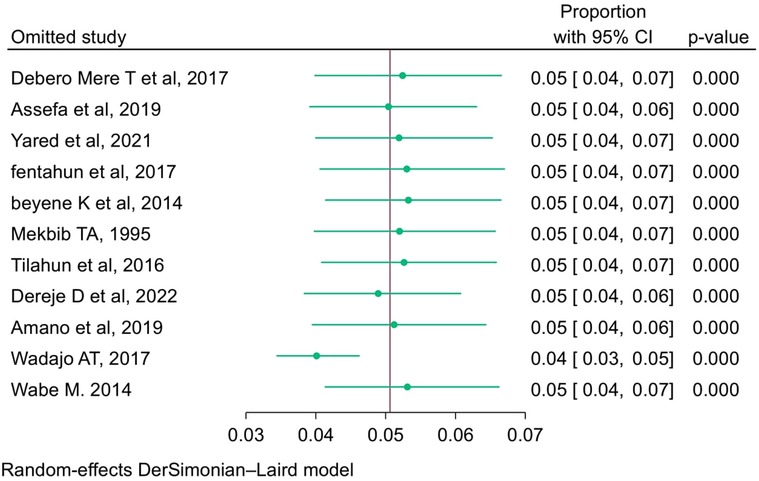
Figure 7. Leave one out meta-analysis of prevalence breech delivery among women in Ethiopica, 2023.
4 DiscussionThe purpose of this systematic review and meta-analysis was to determine the rate of caesarean sections among women who gave breech deliveries in Ethiopia. In this review, the pooled prevalence of breech deliveries among women in Ethiopia was 5% [95% CI: 4, 6]. The overall pooled cesarean section rate among breech deliveries in Ethiopia was 41% (95% CI: 29–54). This finding pointed out that two out of every five pregnant women with breech presentation gave birth by cesarean section in Ethiopia. This is in line with the systematic review and meta-analysis conducted in Nigeria (30). This implies that a large portion of women with breech presentations end up with caesarian deliveries, which in turn predispose the women to various short-term and long-term surgical complications after caesarian sections (31, 32). Thus, as compared to vaginal delivery, pregnant women who gave birth through caesarian delivery were at higher risk for incisional hernia (33, 34), bowel obstruction (35), abdominal pain (36), and organ damage (32). The catastrophic sequels related to complications after caesarean sections are not only limited to the mother but also explicitly affect the neonates. Some of the prominent complications are birth asphyxia, trauma, jaundice, and hypoglycemia (37, 38). Hence, coordinated action and measures need to be taken to mitigate and alleviate potential risk factors that lead to caesarean sections.
According to this systematic review and met analysis, there is a significant difference in the years of publication, which explicitly confirmed the rate of caesarian section among the breech deliveries within the given years of publication. Thus, based on subgroup analysis by publication year, the highest rate of cesarean section in breech deliveries among women in Ethiopia was observed among studies conducted during and before 2014, which was 61% (95% CI: 55–67). Additionally, according to this systematic review and meta-analysis, the rate of caesarian section among breech deliveries showed a bit of a reduction after 2015, which was 57% (95% CI: 41, 72). This is related to the decline in breech delivery, which in turn led to reductions in cesarean sections in the given years.
Moreover, this systematic review and meta-analysis revealed that the rate of caesarean section among breech deliveries enormously varies across regions of the country. Accordingly, the highest rate was reported from the Oromia region, which was 65% (95% CI: 50, 80), whereas the lowest was reported from the Amhara region, accounting for 29% (95% CI: 23, 35). This variation could be attributed to the fact that a number of the original studies were included in reviews. For instance, the review entails five studies from Oromia and one study from the Amhara region. Hence, as ANC visits help in the early identification of breech presentation, they also greatly reduce the consequences of breech presentation, such as caesarian sections (39–41).
5 Strengths and limitations of the studyThe study's strength is that the publications were found in a variety of genuine databases, websites, and institutional repositories. Another strength is that, to the best of the investigators’ knowledge, it is the first SRM on adverse perinatal outcomes in breech deliveries. However, the majority of the pieces came from a few regions. During the article search, only the English language was taken into account. Furthermore, unpublished studies were included in this review and may influence the overall estimate.
6 ConclusionIn this review, the pooled prevalence of breech deliveries among women in Ethiopia was 5%, and the overall rate of caesarian section among the breech deliveries was 41%. This finding pointed out that two out of every five pregnant women with breech presentation gave birth by cesarean section in Ethiopia. Therefore, the finding implies that both the government and all the concerned stakeholders shall be given particular emphasis made on strengthening antenatal care services and ensure more women have access to skilled healthcare professionals during childbirth. This can help in providing appropriate interventions, support to women and reducing the need for emergency and unnecessary CSs. The result of this research are a baseline data for future researchers to conduct further studies to better understand the reasons behind the high rates and identify potential interventions and solutions specific to the African context.
Data availability statementThe original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributionsIM: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. AD: Validation, Writing – original draft, Writing – review & editing. LR: Writing – review & editing. BA: Conceptualization, Methodology, Writing – review & editing. UJ: Conceptualization, Data curation, Formal Analysis, Writing – original draft, Writing – review & editing. AE: Conceptualization, Methodology, Writing – original draft, Writing – review & editing.
FundingThe author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study’s design, data collection, analysis, and interpretation, as well as the development of the paper, are all independent of the sponsor.
AcknowledgmentsWe would like to express our sincere gratitude to Haramaya University for supporting us in writing this work, as well as to the data collectors and supervisors.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary materialThe Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fsurg.2024.1283965/full#supplementary-material
References2. Ngowa JDK, Kasia JM, Ekotarh A, Nzedjom C. Neonatal outcome of term breech births: a 15-year review at the Yaoundé general hospital, Cameroon. Clin Mother Child Health. (2012) 9:0–0.
3. Debero Mere T, Beyene Handiso T, Mekiso AB, Selamu Jifar M, Aliye Ibrahim S, Belato DT. Prevalence and perinatal outcomes of singleton term breech delivery in Wolisso hospital, Oromia region, southern Ethiopia: a cross-sectional study. J Environ Public Health. (2017) 2017:9413717. doi: 10.1155/2017/9413717 Erratum in: J Environ Public Health. 2018 February 26; 2018:2143031. doi: 10.1155/2018/2143031.29333173
PubMed Abstract | Crossref Full Text | Google Scholar
4. Fernández-Carrasco FJ, Cristóbal-Cañadas D, Gómez-Salgado J, Vázquez-Lara JM, Rodríguez-Díaz L, Parrón-Carreño T. Maternal and fetal risks of planned vaginal breech delivery vs planned caesarean section for term breech birth: a systematic review and meta-analysis. J Glob Health. (2022) 12:04055. doi: 10.7189/jogh.12.04055
PubMed Abstract | Crossref Full Text | Google Scholar
5. Hannah ME, Hannah WJ, Hewson SA, Hodnett ED, Saigal S, Willan AR. Planned caesarean section versus planned vaginal birth for breech presentation at term: a randomised multicentre trial. Term breech trial collaborative group. Lancet. (2000) 356(9239):1375–83. doi: 10.1016/S0140-6736(00)02840-3
PubMed Abstract | Crossref Full Text | Google Scholar
6. Wängberg Nordborg J, Svanberg T, Strandell A, Carlsson Y. Term breech presentation-intended cesarean section versus intended vaginal delivery-a systematic review and meta-analysis. Acta Obstet Gynecol Scand. (2022) 101(6):564–76. doi: 10.1111/aogs.14333
PubMed Abstract | Crossref Full Text | Google Scholar
7. Derisbourg S, Costa E, De Luca L, Amirgholami S, Bogne Kamdem V, Vercoutere A, et al. Impact of implementation of a breech clinic in a tertiary hospital. BMC Pregnancy Childbirth. (2020) 20(1):435. doi: 10.1186/s12884-020-03122-4
PubMed Abstract | Crossref Full Text | Google Scholar
10. Zakerihamidi M, Latifnejad Roudsari R, Merghati Khoei E. Vaginal delivery vs. cesarean section: a focused ethnographic study of women’s perceptions in the north of Iran. Int J Community Based Nurs Midwifery. (2015) 3(1):39–50.25553333
PubMed Abstract | Google Scholar
11. Waterfall H, Grivell RM, Dodd JM. Techniques for assisting difficult delivery at caesarean section. Cochrane Database Syst Rev. (2016) 2016(1):CD004944. doi: 10.1002/14651858.CD004944.pub3
PubMed Abstract | Crossref Full Text | Google Scholar
12. Smith BA. Anesthesia as a risk for health care acquired infections. Perioper Nurs Clin. (2010) 5(4):427–41. doi: 10.1016/j.cpen.2010.07.005
Crossref Full Text | Google Scholar
15. Njim T, Tanyitiku BS, Mbanga C. Prevalence, indications and neonatal complications of caesarean deliveries in Cameroon: a systematic review and metaanalysis. Arch Public Health. (2020) 78:51. doi: 10.1186/s13690-020-00430-1
PubMed Abstract | Crossref Full Text | Google Scholar
17. Jejaw M, Teshale G, Yazachew L, Dellie E, Debie A. Adverse birth outcome among women who gave birth at the University of Gondar comprehensive specialized hospital, northwest Ethiopia. BMC Pregnancy Childbirth. (2024) 24(1):285. doi: 10.1186/s12884-024-06478-z
PubMed Abstract | Crossref Full Text | Google Scholar
18. Tilahun T, Mengistie H, Hiko D. Prevalence and perinatal outcome of singleton term breech delivery in Mizan Aman general hospital, south west, Ethiopia; a three year retrospective hospital based study. J Women’s Health Care. (2016) 5(319):34–9. doi: 10.4172/2167-0420.100031916
Crossref Full Text | Google Scholar
19. Mekbib TA. Breech delivery and foetal outcome: a review of 291 cases. Ethiop Med J. (1995) 33(3):175–82.7588656
PubMed Abstract | Google Scholar
20. Peterson J, Welch V, Losos M, Tugwell PJ. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa: Ottawa Hospital Research Institute. (2011) 2(1):1–12
21. Tadesse A, Araya F, Dube L. Determinants of breech presentation at birth in singletons at Jimma university medical center, south west Ethiopia: a case-control study. (2017). doi: 10.140.5.162/handle/123456789/2794
Crossref Full Text | Google Scholar
22. Hibestie F. Perinatal outcome of singlton breech delivery at Yirgalem General Hospital, SNNPR, Ethiopia: A Cross-Sectional Study. J Environ Public Health. (2017) 2017:9413717.
23. Adebami OJ, Owa JA, Oyedeji GA, Oyelami OA. Prevalence and problems of foetal malnutrition in term babies at Wesley guild hospital, south western Nigeria. West Afr J Med. (2008) 26(4):278–82. doi: 10.4314/wajm.v26i4.28327
Crossref Full Text | Google Scholar
24. Sume BW. Fetal malnutrition and associated factors among newborn babies delivered at Debre Markos comprehensive specialized hospital, Ethiopia. Int J Africa Nurs Sci. (2023) 18:100543. doi: 10.1016/j.ijans.2023.100543
Crossref Full Text | Google Scholar
26. Assefa F, Girma W, Woldie M, Getachew B. Birth outcomes of singleton term breech deliveries in Jimma university medical center, southwest Ethiopia. BMC Res Notes. (2019) 12(1):428. doi: 10.1186/s13104-019-4442-6
PubMed Abstract | Crossref Full Text | Google Scholar
27. Wabe M. Prevalence and Fetal Outcome of Singleton Breech Delivery at Tercha General Hospital, SNNPRS, Ethiopia. Jimma: Jimma University (2014).
28. Koo MR, Dekker GA, van Geijn HP. Perinatal outcome of singleton term breech deliveries. Eur J Obstet Gynecol Reprod Biol. (1998) 78(1):19–24. doi: 10.1016/S0301-2115(97)00278-9
PubMed Abstract | Crossref Full Text | Google Scholar
29. Jaleta DD, Abdisa DK. Predictors of adverse perinatal outcome among women who gave birth at medical center of southwest Ethiopia: a retrospective cohort study. BMJ Open. (2022) 12(3):e053881. doi: 10.1136/bmjopen-2021-053881
PubMed Abstract | Crossref Full Text | Google Scholar
30. Tunau K, Ahmed Y. Breech deliveries in Usmanu Danfodiyo university teaching hospital Sokoto, northwestern Nigeria: a 10-year review. Sahel Med J. (2013) 16:52–5. doi: 10.4103/1118-8561.115257
Crossref Full Text | Google Scholar
31. Green JE, McLean F, Smith LP, Usher R. Has an increased cesarean section rate for term breech delivery reduced in incidence of birth asphyxia, trauma, and death? Am J Obstet Gynecol. (1982) 142(6 Pt 1):643–8. doi: 10.1016/S0002-9378(16)32434-6
PubMed Abstract | Crossref Full Text | Google Scholar
32. Larsson C, Djuvfelt E, Lindam A, Tunón K, Nordin P. Surgical complications after caesarean section: a population-based cohort study. PLoS One. (2021) 16(10):e0258222. doi: 10.1371/journal.pone.0258222
PubMed Abstract | Crossref Full Text | Google Scholar
33. Paulsen CB, Zetner D, Rosenberg J. Incisional hernia after cesarean section: a systematic review. Eur J Obstet Gynecol Reprod Biol. (2020) 244:128–33. doi: 10.1016/j.ejogrb.2019.11.010
PubMed Abstract | Crossref Full Text | Google Scholar
35. Visser A, Geboers B, Gouma DJ, Goslings JC, Ubbink DT. Predictors of surgical complications: a systematic review. Surgery. (2015) 158(1):58–65. doi: 10.1016/j.surg.2015.01.012
PubMed Abstract | Crossref Full Text | Google Scholar
36. Andolf E, Thorsell M, Källén K. Cesarean delivery and risk for postoperative adhesions and intestinal obstruction: a nested case-control study of the Swedish medical birth registry. Am J Obstet Gynecol. (2010) 203(4):406.e1–6. doi: 10.1016/j.ajog.2010.07.013
PubMed Abstract | Crossref Full Text | Google Scholar
37. Chawanpaiboon S, Titapant V, Pooliam J. Neonatal complication of caesarean sections at tertiary center: Siriraj hospital, Bangkok, Thailand. Afr J Reprod Health. (2022) 26(9):118–32. doi: 10.29063/ajrh2022/v26i9.12
PubMed Abstract | Crossref Full Text | Google Scholar
38. Kamath BD, Todd JK, Glazner JE, Lezotte D, Lynch AM. Neonatal outcomes after elective cesarean delivery. Obstet Gynecol. (2009) 113(6):1231–8. doi: 10.1097/AOG.0b013e3181a66d57
留言 (0)