
記住我
Medical rules and guidelines play crucial roles in various aspects of dermatology and clinical practice, offering structured approaches to assessment, diagnosis, and treatment. These rules are designed to enhance diagnostic accuracy, optimise therapeutic interventions, and improve patient outcomes across different dermatological conditions. We present a concise overview of several important rules and their applications:
Rules for skin cancer ABCDE ruleThis method is used to assess whether a mole is benign or malignant. It has asymmetry, border irregularity, colour variation, diameter > 6 mm, and evolution.1
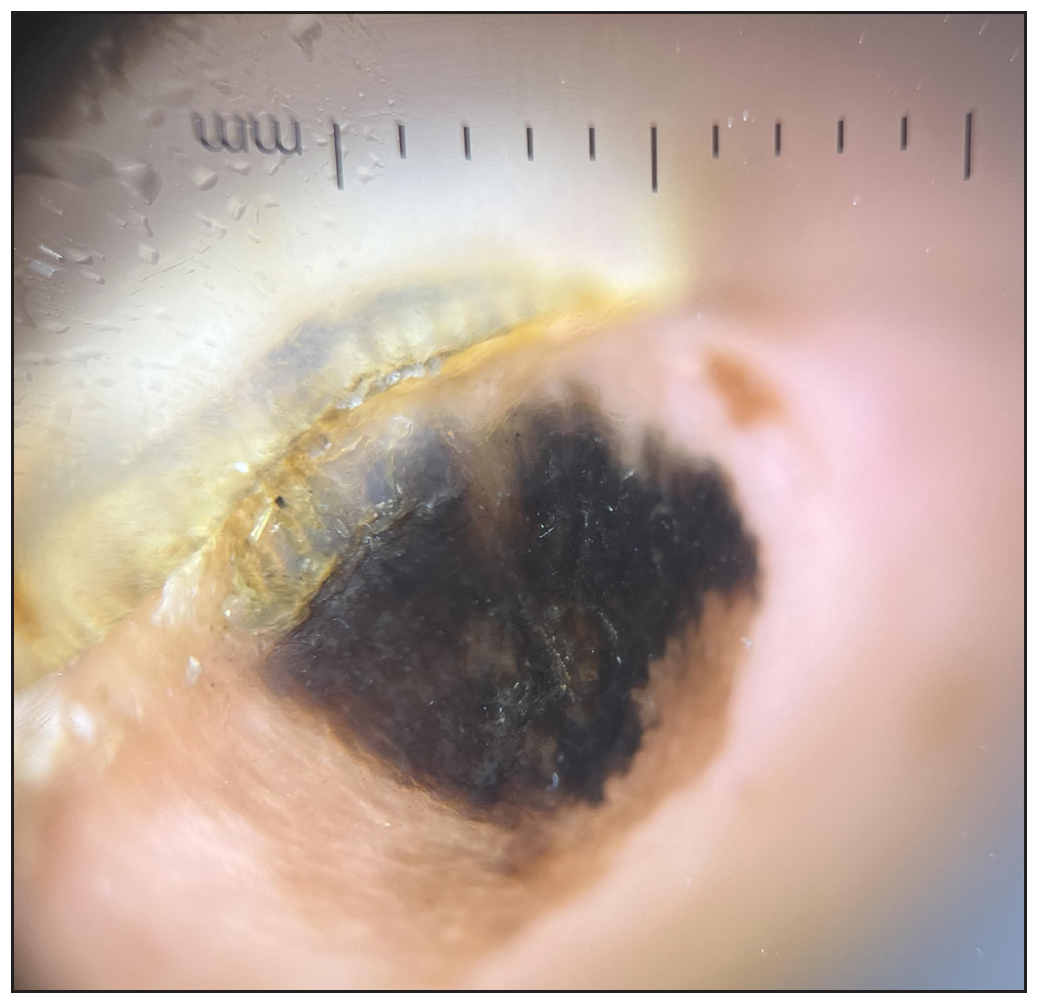
ABCDEF ruleThis is used for subungual melanoma diagnosis. It includes age (fifth to the seventh decade); brown/black colour, band ≥3 mm; change in size/morphology; affected digit; pigment extension onto nail fold; and familial/personal melanoma/dysplastic naevi history.2
Rule of 10s and 2s for melanoma excisionSpecialty site melanomas on the head and neck, hands and feet, genitalia, and pretibial leg have higher rates of surgical complications after conventional excision with postoperative margin assessment (CE-POMA) compared with trunk and proximal extremity melanomas. The rule of 10s describes complication rates after CE-POMA of specialty site melanomas: ∼10% risk for upstaging, ∼10% risk for positive excision margins, ∼10% risk for local recurrence, and ∼10-fold increased likelihood of reconstruction with a flap or graft. . This statistic underscores the challenges of managing melanomas located in anatomically complex or cosmetically sensitive areas. The 10% risk of upstaging indicates that even after excision, the tumour may be found to be more advanced than initially diagnosed, necessitating further intervention or monitoring. Moreover, the tenfold increase in the likelihood of requiring reconstructive procedures with flaps or grafts highlights the need for careful surgical planning and expertise in these regions. Trunk and proximal extremity melanomas encounter these complications at a lower rate, according to the rule of 2s.3
Rule of genetic testing in melanomaThis rule is used to select melanoma patients for genetic testing [Table 1], according to the incidence of melanoma in the general population and the prevalence of mutations.4
Table 1: Rules for genetic testing for melanoma
Rule of 2 Rule of 3 Rule of 4 Low melanoma incidence countries Moderate to high-incidence countries Very high-incidence countries1. Individuals with two primary melanomas or a family with one invasive melanoma
2. Pancreatic cancers among first or second generation
1. Individuals with three primary invasive melanomas
2. Family with one invasive melanoma
3. 2 cases of pancreatic cancers among first or second generation
Ten seconds rule for melanomaThe ‘ten-second rule’ is a guideline for evaluating single melanoma lesions to distinguish benign from malignant growths. It suggests that an experienced dermoscopist can often diagnose a lesion as benign or malignant within a few seconds if clear, recognisable features are present. However, if an examination takes longer than ten seconds due to ambiguous features, it indicates enough diagnostic uncertainty to consider excision or biopsy for a definitive diagnosis. It prompts excision for diagnosis when lesions exhibit unspecific patterns, atypical networks, extensive regression, or peripheral streaks. Unspecific patterns suggest irregularity, while atypical networks indicate malignancy. Extensive regression can mask cancerous changes and peripheral streaks may signal invasion into the surrounding tissues. This rule aids clinicians in making timely decisions, enhancing diagnostic accuracy, and facilitating early intervention.5
Three-point dermoscopy ruleThe three-point dermoscopy rule Figure 1 identifies dermoscopic asymmetry (in terms of colour and structure rather than the shape), atypical network patterns (a pigmented network characterised by thick lines and irregular distribution) and blue-white structures (any presence of blue and white colouration within the lesion). According to the three-point checklist, the presence of two or more of these features indicates a malignancy.6
Export to PPT
Rules for infections Rule of two for dermatophytosisWhen using topical antifungal treatments for dermatophytosis, it is essential to emphasise the following: ensure regular application, adhere strictly to medical advice, extend application 2 cm beyond the lesions twice daily, and continue treatment for two weeks after clinical resolution.7
90-60 rule for candidiasisAlthough antifungal resistance is usually correlated with increased minimum inhibitory concentration (MIC). MIC values do not always correlate with clinical response to antifungal drugs. This discordance between the in vivo and in vitro resistance in candidiasis has been illustrated by the “90–60 rule”. Infections due to susceptible strains respond to appropriate therapy in 90% of cases, whereas infections due to resistant strains respond in approximately 60% of patients.7
Rules for cosmetic procedures Jenkin’s rule of suturingThe length of the suture used should be four times the length of the wound to ensure adequate coverage for effective closure. Sutures should be spaced approximately 1 cm apart along the wound, with each suture taking a 1 cm bite of the wound edge. These guidelines help prevent increased tension, promote optimal healing, and reduce wound complications.8
Rule of five for poly-L-lactic acid injectionTo minimise papule formation after injecting poly-L-lactic acid, it is essential to incorporate a specific post-injection protocol involving a firm massage of the treated area. The recommended approach is to massage the area firmly for five minutes, five times daily, for a total of five days following the injection. This technique serves a dual purpose: it helps ensure even dispersion of the poly-L-lactic particles within the dermal layer and reduces the likelihood of localised swelling or nodularity.9
Rule of halves for curvilinear incisionsCurvilinear incisions often result in dog ear formation due to uneven wound lengths. The rule of halves technique effectively prevents this issue. A modified version ensures a cosmetically pleasing outcome by redistributing length discrepancies towards the wound’s centre.10
Rules for pharmacological guidelines Five hundred dalton rule for skin absorptionA molecular weight of under 500 Daltons facilitates skin absorption during transdermal delivery in topical therapy. This criterion also applies to common allergens, as larger molecules have limited skin penetration and sensitisation potential. Size is pivotal in skin absorption and allergenicity, guiding substance selection for effective treatments.11
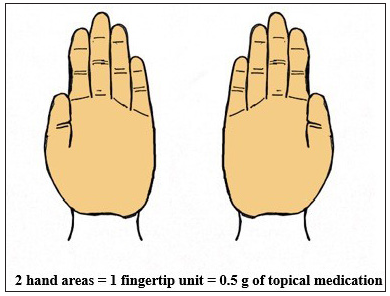
Rule of hand for topical steroid applicationRule of hand [Figure 2] is used to optimise the use of steroids (topical steroid application). This rule states that an area of the size that can be covered by four adult hands (including digits) can be treated by 1gm or two fingertip units.12
Export to PPT
Teaspoon rule for sunscreen applicationSunscreen application guidelines recommend using a little more than half a teaspoon (3 mL) for each of the head and neck, right arm, and left arm. For the anterior and posterior trunk areas as well as each leg, applying little more than a teaspoon is advised. This ensures adequate coverage and protection from ultraviolet radiation.13
80:20 rule for drug interactionsDrug interactions tend to be predictable and adhere to the principle that roughly 20% of medications are responsible for 80% of all interactions.14
Body surface area rules Rule of four for facial assessmentThis method offers a reliable and accurate assessment of facial areas. The ‘rule of fours’ correlates well with image analysis, defining facial regions as percentages of the total area: forehead (24%), one cheek (20%), perioral area (8%), one ear aspect (4%), one periorbital area (4%) and nose (4%).15 These percentage values are approximate, based on a specific model, and may vary slightly by age and population.
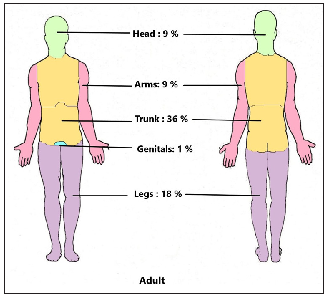
Rule of nines (Wallace rule of nines)The rule of nines [Figure 3] is used to assess the total body surface area affected in burn patients and estimate the required fluid for resuscitation to restore lost fluids.16
Export to PPT
Rule of ten (Finlay’s rule)This is utilised to identify severe psoriasis when the body surface area involved is greater than 10%, when the Psoriasis Area and Severity Index exceeds 10, or when the Dermatology Life Quality Index score is above 10.17
Rule of thumb for scalp surface areaThe thumbprint, averaging 5.5 cm2 × 1.3 cm2, serves as a practical tool to assess 1% scalp surface area, aligning well with the range of 5.2 cm2–7.1 cm2 in clinical visual assessments.18
Miscellaneous rules Clinical prediction rule for nerve-function impairment in leprosyThe prediction of nerve-function impairment in new leprosy cases is based on three critical factors identified through multivariable Cox regression analysis: the leprosy group (multibacillary or paucibacillary), the presence of existing nerve-function loss and the detection of nerve-trunk enlargement at the time of registration.19
Rule of four R’s for hand eczemaThe four R’s rule is applied in the management of hand eczema and encompasses four key components: the recognition of the causative irritant or allergen, the removal of the identified irritant or allergen, the reduction of skin inflammation, and the restoration of the skin barrier.20
5R + R rule for actinic keratosisThe 5R + R rule for actinic keratosis helps identify predictive factors that aid in the early detection, treatment, and prevention of the condition, thereby reducing the risk of recurrence and progression to malignancy. The factors include: ‘reddish’, which emphasises the importance of visualising the lesion; ‘rough skin’, which refers to texture and thickness, aiding in clinical grading; ‘cephalic region’, indicating areas frequently exposed to ultraviolet radiation; and ‘ultraviolet radiation exposure’, which is identified as the main risk factor. Additionally, ‘recurrence’ highlights the need for ongoing monitoring, while the final ‘+R’ signifies the risk of malignant transformation, underscoring the importance of early and effective management.21
ConclusionVarious medical rules and guidelines in dermatology provide structured frameworks that simplify and enhance clinical decision-making, ensuring that practitioners can deliver consistent and effective care. For instance, the ABCDE and ABCDEF rules offer straightforward yet vital criteria to distinguish benign from malignant lesions, facilitating early diagnosis and timely intervention in skin cancer cases. Similarly, guidelines like the ‘rule of two’ for dermatophytosis and the ‘rule of hand’, for topical steroid application emphasise proper drug usage, dosage, and adherence that is crucial for the effective treatment and prevention of recurrence. Cosmetic procedures also benefit from rules that minimise complications, such as Jenkins’ rule for suturing and the rule of halves for curvilinear incisions, improving aesthetic outcomes and patient satisfaction. These rules collectively contribute to a more holistic understanding of patient management, allowing a correct diagnosis, efficient treatment, and negligible therapy-associated complications. By promoting adherence to standardised protocols, they support uniformity in practice, which is essential for both patient safety and the advancement of evidence-based dermatology.
留言 (0)