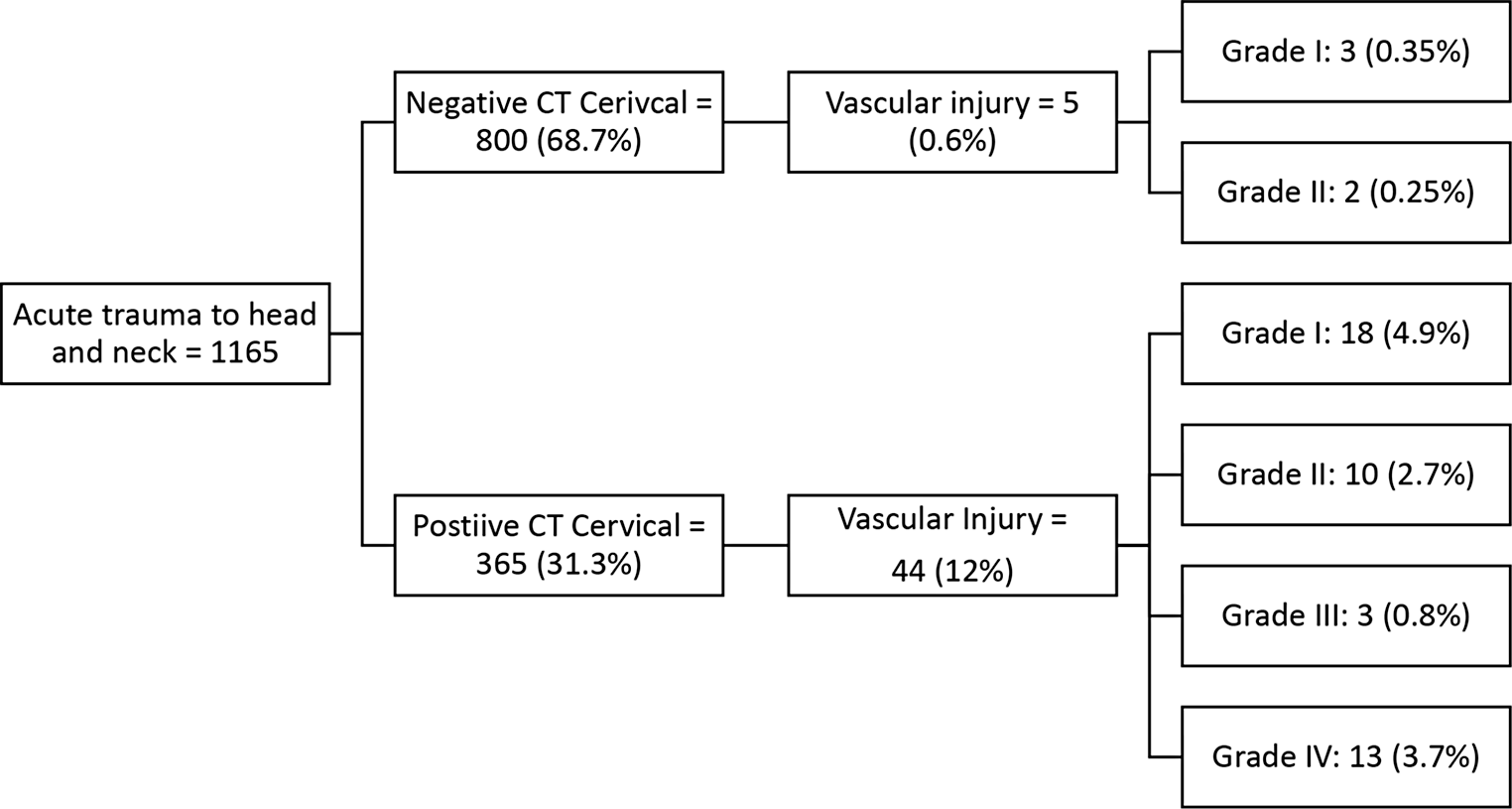
The current study offers significant insights into the incidence and severity of cervical vascular injuries following blunt cervical trauma in patients who show no fractures on cervical CT scans. Only 0.6% of those patients sustained vascular injury visible on CTA, and no recorded injuries above grade II. This is in contrast to a 12% risk of vascular injury in patients with positive cervical CT scans. Our findings suggest that routine CTA might not be necessary in patients who lack visible signs of cervical fractures on initial imaging, and should be considered more selectively, based on specific clinical presentations rather than as a standard response.
The potential for cervical vascular injuries following blunt trauma is notably high, with general risks estimated up to 11%, and increasing to as much as 30% when a cervical fracture is present [6, 7]. The incidence in our cohort was 12%. Such injuries are critically important to identify promptly as they can lead to ischemic strokes. These strokes often remain clinically undetected, especially in scenarios where patients are intubated and undergoing multiple interventions due to polytrauma. In these cases, CTA serves as a crucial diagnostic tool to swiftly identify vascular injuries even when overt clinical symptoms are absent, enabling the initiation of preventive therapies aimed at mitigating the progression of ischemia [7]. Furthermore, specific fracture types such as those extending into the transverse foramen dramatically increase the risk of vertebral artery injuries. Likewise, vertebral dislocations, including those involving jumped facets, can cause sudden shifts around the anchored vertebral artery within the foramen, potentially leading to dissections or other forms of injury [8].
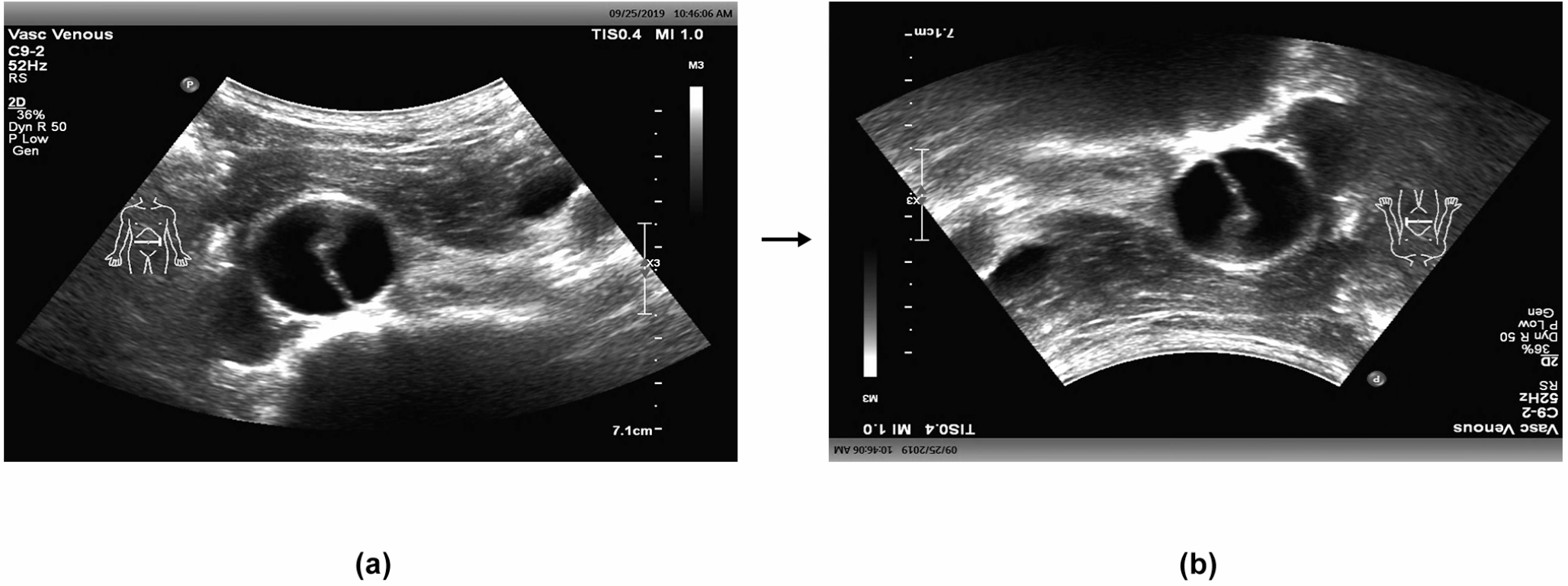
This study appears to be the first to quantify the incidence of cervical vascular injuries among patients who have sustained blunt cervical trauma yet show no fractures on CT scans. The predominant mechanism of injury in these cases likely involves excessive shearing forces experienced during extreme movements, such as the rapid flexion and extension seen in whiplash injuries. This dynamic can result in intimal damage to the vascular walls, which was supported by our findings where all affected patients exhibited only grade I or II injuries [9].
These findings also highlight the current practice of performing CT cervical spine imaging and CTA concurrently, a method that has become widespread due to its efficiency in trauma settings. However, this approach raises important considerations regarding radiation exposure, patient transport logistics, and overall workflow management in emergency departments. While the simultaneous use of CT and CTA offers advantages in speed and comprehensive assessment, it also results in higher cumulative radiation doses to patients. This concern is particularly relevant when the CTA may not yield significant clinical findings, as shown by our study’s results: only 0.6% of patients without fractures on initial CT scans exhibited vascular injuries, and all identified injuries were limited to grade I or II severity. These findings suggest that routine use of CTA should be more selectively applied, especially in cases without evidence of fractures.
This study has two key implications: first, it questions the routine use of CTA when CT scans do not show fractures, advocating instead for a more selective approach based on clinical judgment and individual patient factors. Second, it highlights the need to identify subtle but potentially serious vascular injuries in patients with significant blunt cervical trauma. This refined understanding can lead to more precise and effective clinical interventions, ultimately improving outcomes for this challenging group of trauma patients.
Limitations
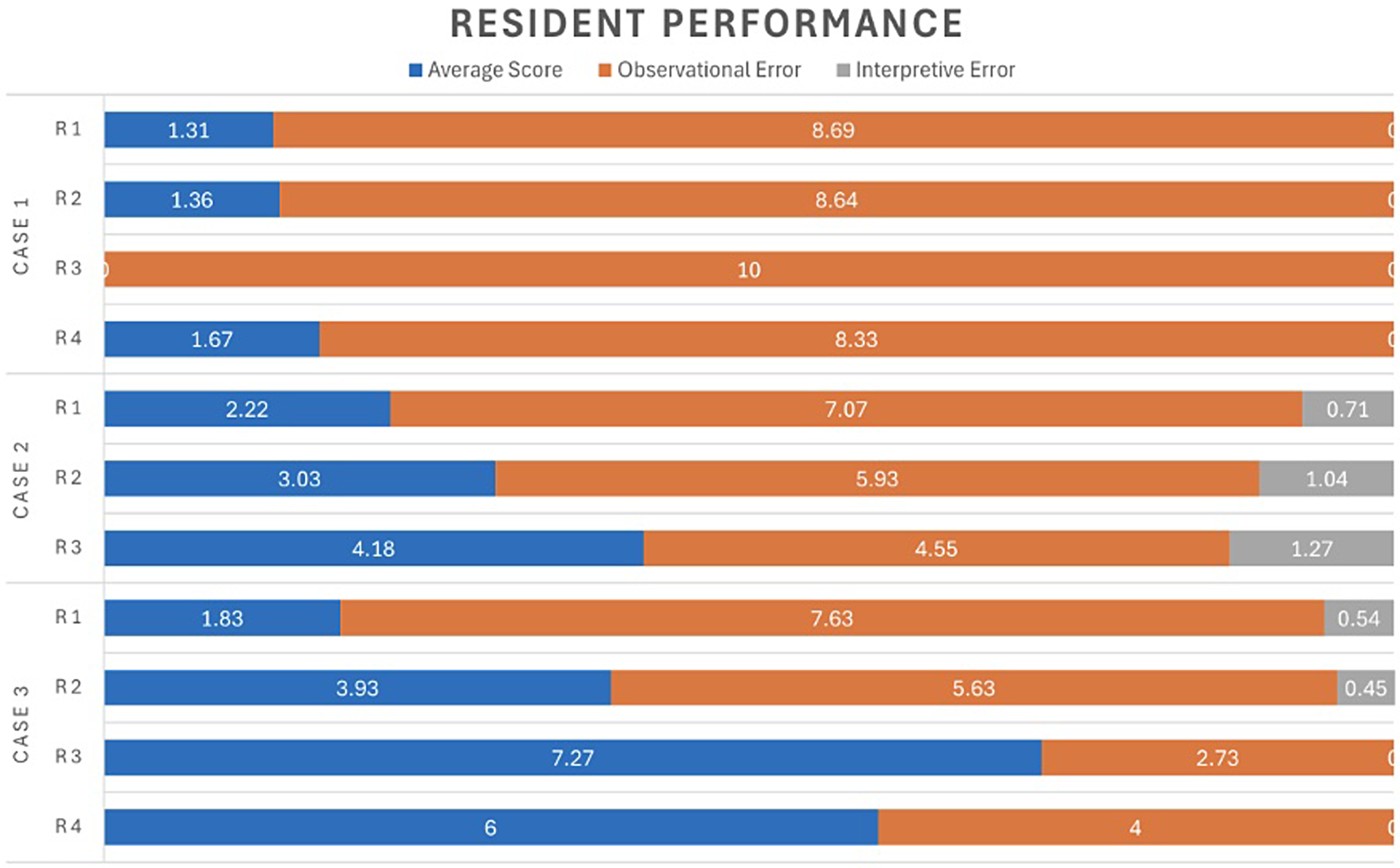
The study presents some limitations that must be considered when interpreting the findings. Firstly, the retrospective design of the study inherently limits our ability to control for all potential confounding variables that might influence the outcomes. Another significant limitation is the single-center nature of the study. The data was collected from only one hospital, which may limit the generalizability of the results. Hospitals vary in patient demographics, trauma severity, and clinical practices. Additionally, the interpretation of imaging studies in our research was conducted by multiple radiologists whose levels of experience varied. This variation could lead to inconsistencies in the interpretation of CT and CTA scans, potentially affecting the reliability of the data on detected injuries. Differences in diagnostic accuracy and observational skills among radiologists might result in either overestimation or underestimation of the prevalence of vascular injuries in the studied population.



留言 (0)