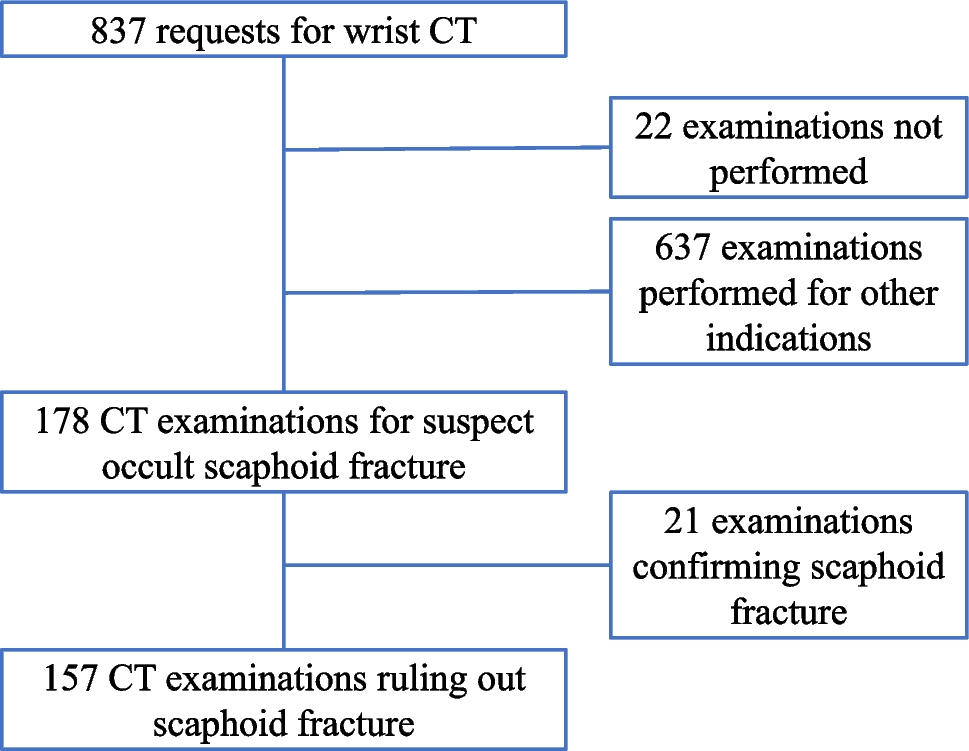
In the current study, there were no late complications from scaphoid fractures missed at CT. One scaphoid fracture was missed at initial reporting, but was detected the following day, and in the current study was detected on the blinded study review. Thus, it would appear that CT is a good enough method to evaluate suspect radiographically occult scaphoid fractures.
A missed occult scaphoid fracture has the potential for severe complications, such as AVN or pseudarthrosis, leading to SNAC. Every patient with pseudarthrosis will probably eventually develop SNAC, even after several decades. Therefore, all patients with remaining clinical signs of scaphoid fracture after radiography are usually treated with a cast until follow-up imaging has been done. This means that about 80% of patients with scaphoid trauma may be treated unnecessarily [28,29,30]. Recent guidelines [21] published after the patients in the current study were examined recommend early follow-up imaging with primarily MRI, stating CT as a reliable alternative in the absence of MRI, supported by the findings in the current study. A recent report analyzing the cost-effectiveness of various regimens suggests that immediate CT or MRI bypassing radiography are the most cost-effective ways to evaluate a suspected scaphoid fracture [31], something that has been implemented in many institutions.
MRI is usually advocated as the follow-up imaging of choice [14, 21] due to its high sensitivity. However, treatment of purely trabecular fractures at MRI may be unnecessary and potentially harmful, with possible complications arising from immobilization in cast. Differentiation between bone marrow edema and a true fracture with potential for displacement is difficult [26] with different studies having applied different definitions [16, 26]. A purely trabecular fracture without cortical fracture should not be regarded as a potentially unstable fracture, nor should an avulsion fracture of the scaphoid tubercle. Since the exact distinction between trabecular and cortical fractures at MRI has not been made, it would be unethical to perform a scientific study where scaphoid fractures at MRI are randomized to treatment with a cast for at least six weeks or to symptomatic treatment. The current study tries to address this predicament by using the approach that purely trabecular fractures at MRI would not show up at CT and were thus not treated more than symptomatically in the current study. None of these supposed cases showed progression into a displaced scaphoid fracture. However, since 124 of 157 patients wore a cast in the period preceding CT, and 48 patients were immobilized for a certain time after CT with a plaster cast or removable splint, it is not inconceivable that patients with non-displaced scaphoid fractures that had been occult on CT were included in this group. This treatment group also includes patients with other wrist or carpal bone fractures, patients with presumed ligamentous injuries, and patients receiving treatment for residual wrist pain. The combination of modern treatment, including wrist immobilization for pain until follow-up imaging and modern high-quality CT, thus seems adequate for diagnosis and treatment of suspected occult scaphoid fracture. During recent years, CBCT has come to be employed for primary diagnosis of scaphoid fracture in many institutions [17, 32], showing high sensitivity for scaphoid fracture at a lower radiation dose than imaging with a whole-body CT scanner [33], and having a higher spatial resolution. However, the number of suitable patients needs to be large enough to motivate the purchase of a specialized extremity CT.
During the study period, CT was the follow-up imaging of choice in case of suspect scaphoid fractures at the authors’ institution. At the end of the study period, increasingly more follow-up imaging was made with MRI. MRI has the potential ability to detect other reasons for post-traumatic radial sided wrist pain, such as other fractures or bone contusions, soft tissue contusions, and possibly ligamentous injuries [30]. In the current study, other fractures than a scaphoid fracture was detected in 29 patients without a scaphoid fracture, a prevalence of 18%. Other fractures than of the scaphoid have also been reported at scaphoid MRI [23]. A high prevalence of ligamentous injuries concomitant with scaphoid fracture has been reported at wrist arthroscopy [34]. It is also worth noting the sex difference in patient inclusion and fracture prevalence, with more women examined than men, but men having a significantly higher scaphoid fracture rate.
The strengths of the study are the large number of patients and long available follow-up time in the PACS archive and the medical records to detect possible complications from a missed scaphoid fracture on CT with later displacement. The limitations of the study are the retrospective nature, the lack of comparative imaging with MRI, not having dedicated scaphoid long-axis CT reformations, and not using dynamic multi-planar reformations (MPR) at the primary reading, which was not available in the clinical PACS at the time. A significant limitation which limits the conclusions to be drawn from the study is the fact that most patients received treatment with a plaster cast or a splint before CT, and many also for a time after CT as pain treatment, which makes it impossible to exclude that some non-displaced fractures may have healed during this treatment.
In conclusion, the current study revealed no missed occult scaphoid fractures at follow-up CT after normal radiography, suggesting that CT may be a reliable method for evaluating suspect scaphoid fracture as part of a diagnosis-treatment regimen including pain immobilization with a plaster cast. A randomized controlled study comparing the diagnostic value of CT and MRI treating only patients with cortical fractures at CT is warranted.



留言 (0)