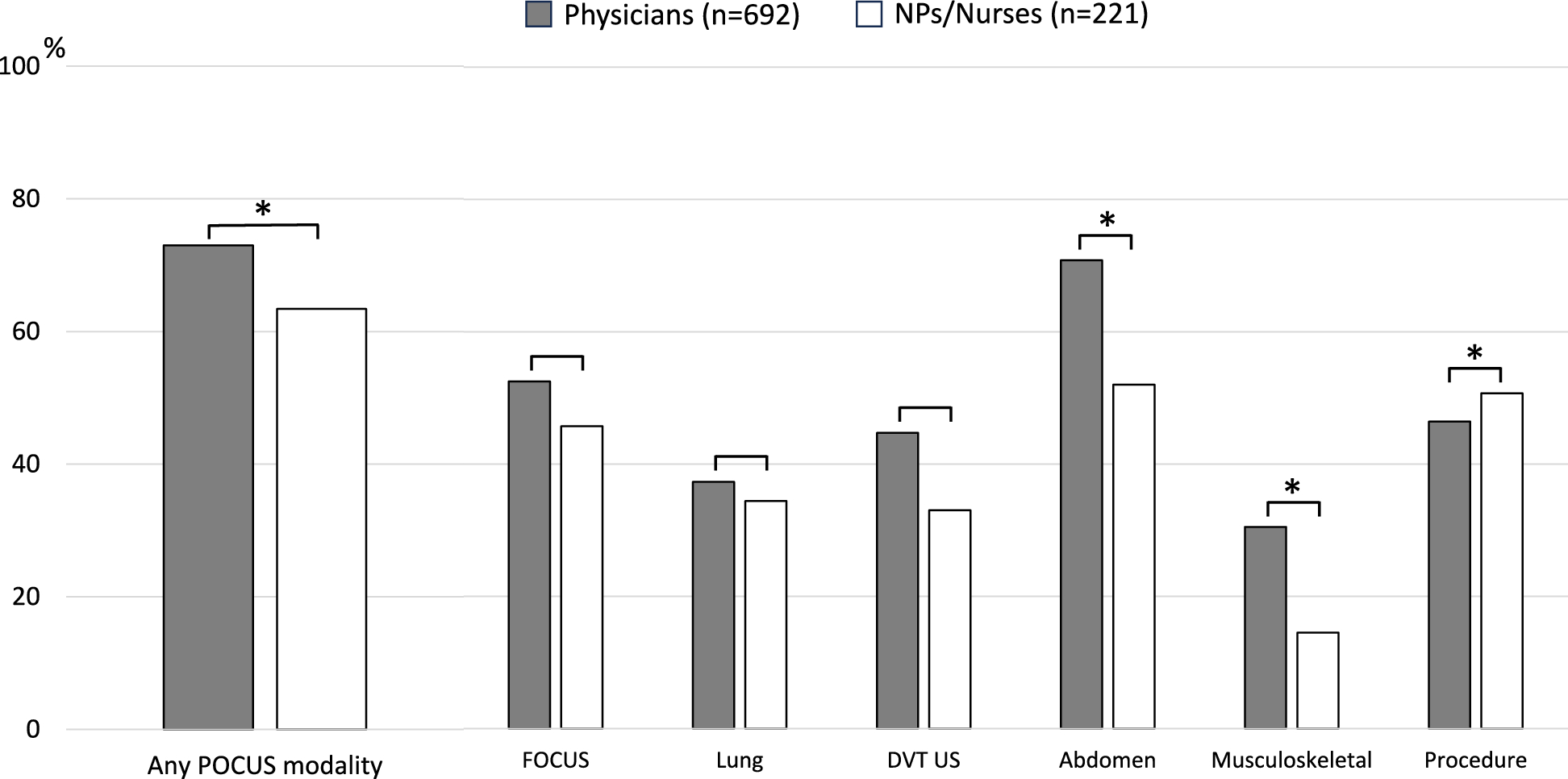
This study investigated the barriers and facilitators to POCUS implementation among 913 physicians, NPs, and nurses. POCUS was used in daily clinical practice by 73.0% of physicians and 63.4% of NPs/nurses. There were no significant differences between physicians and NPs/nurses in the proportions performing FOCUS, lung, or DVT ultrasound. However, the proportion was significantly higher for physicians in abdominal and musculoskeletal ultrasound, while NPs/nurses had a higher proportion for ultrasound-guided procedures. The rankings of essential POCUS skills were similar for both groups, with lung (5th) and musculoskeletal (6th) ultrasound rated as lower priorities among the six skills.
Compared with physicians, barriers for NPs/nurses were significantly more closely associated with a lack of mentors, insufficient image interpretation skills, lack of confidence, limited access to equipment, and the absence of clear policies. In terms of facilitators, NPs/nurses expressed a greater need for support from nearby mentors, adequate institutional support, and official certification of POCUS skills than did physicians. These findings suggest that environmental factors, such as equipment availability, institutional policies, and mentorship, have a greater influence on NPs and nurses than on physicians when implementing POCUS.
Study population and frequency of POCUS use
In this survey, 70.7% of all respondents (physicians: 73.0%, NPs/nurses: 63.4%) reported using some form of POCUS in their routine clinical practice. Among physicians, the most commonly performed POCUS was abdominal ultrasound (70.8%), followed by FOCUS (52.5%), procedures (46.4%), and DVT ultrasound (44.7%). Utilization rates for lung ultrasound (37.3%) and musculoskeletal ultrasound (30.5%) were both in the 30% range. These rates are higher than those in previous reports in the fields of primary care and hospital medicine, which were the main areas of practice for the respondents, as well as past reports from Japan [4, 5, 7, 8]. Based on these findings, it is considered that this survey reflects the perspectives of a group of physicians who actively perform POCUS.
Few studies to date have addressed POCUS implementation by NPs or nurses. POCUS is commonly used by NPs and advanced practice registered nurses in emergency and critical care settings for confirming endotracheal intubation, performing pediatric lung ultrasound, and evaluating ectopic pregnancies [9, 10, 12, 18]. It is also used at the bedside for guiding hemodialysis access and evaluating the inferior vena cava [11, 19]. The need for POCUS is increasingly being emphasized in the care of older adults, a field that is expected to grow rapidly in aging societies [13]. However, the extent to which POCUS is used in each of these areas remains unclear, making it difficult to compare the frequency of POCUS use by NPs and nurses in this survey with that in previous reports. Nonetheless, the fact that the reported frequency in this study does not significantly differ from that of physicians suggests that the responses came from a group of NPs and nurses who actively perform POCUS.
The most common primary specialty for both physicians and NPs/nurses was family medicine, with 80% of respondents working in clinics or community hospitals and more than half engaged in outpatient care. These findings suggest that the responses reflect a group of physicians and NPs/nurses who actively use POCUS in primary care settings.
Both the implementation frequency and perceived necessity for lung and musculoskeletal ultrasound were low. In a survey of 241 participants from 62 low- and middle-income countries (excluding Japan), lung ultrasound was the most frequently indicated modality (58%), followed by cardiac, abdominal, and vascular ultrasound [20]. In the field of hospital medicine in the United States, lung ultrasound is used at a frequency comparable to that of abdominal ultrasound [7]. However, a previous report from Japan indicated that the frequency of lung ultrasound was 5% before training and 17% after training, which was lower than the frequency of other modalities [8]. In this study, the frequency of lung ultrasound was in the 30% range but still lower than that of other modalities. This relatively lower frequency of lung ultrasound in Japan may be a unique characteristic, and the reasons for this are unclear, warranting further investigation.
The proportion of users was higher among NPs/nurses for ultrasound-guided procedures (50.7 vs. 46.4%, p < 0.001). Several reasons may explain this. First, among respondents, the largest proportion of physicians (46.0%) worked in family medicine departments (compared to 23.1% for NPs/nurses), while NPs/nurses had a combined total of 39.8% in EM, CCM, and surgical specialties (compared to only 8.6% for physicians). This suggests that NPs/nurses may have had more opportunities to perform procedures. Additionally, PICC placement is considered a key procedure for NPs [15, 17], which may lead them to take a more active role as practitioners in settings where NPs are present. However, further investigation is needed to confirm this.
Barriers and facilitators
The most frequently cited barrier was the lack of POCUS training opportunities, consistent with previous reports from multiple countries indicating that this is a major factor hindering POCUS utilization [6,7,8, 20, 21]. No significant differences were observed between physicians and NPs/nurses. Factors related to acquiring POCUS competency include image acquisition skills, image interpretation skills, and confidence in performing the procedure [22, 23]. In this survey, a lack of image acquisition skills was the second most common barrier, with no significant differences between physicians and NPs/nurses. However, image interpretation skills and confidence were significantly greater barriers for NPs/nurses than for physicians.
POCUS is most effective when images are interpreted alongside other clinical findings and the patient’s medical history [1]. Therefore, differences between physicians and NPs/nurses in skills and confidence in image interpretation may stem from variations in training backgrounds related to history-taking and pathophysiology, as well as differences in focus and priorities during routine clinical practice. [9, 18]. Additionally, because NPs/nurses may perform ultrasound less frequently than physicians, their lack of familiarity with conducting POCUS could contribute to anxiety about performing the procedure. Previous studies have shown that a lack of confidence is a barrier to POCUS implementation among nurses [19]. Furthermore, in this survey, a lack of supervisors and unclear institutional policies were found to be significantly greater barriers for NPs/nurses than for physicians, emphasizing the importance of having accessible supervisors and institutional or certification program support as facilitators. It is presumed that many institutions lack established protocols for NPs and nurses to perform POCUS independently [12], and these environmental factors may further contribute to their lack of confidence.
Acquiring POCUS skills can enable NPs and nurses to perform earlier and more accurate screening [9,10,11]. Additionally, studies have shown that when NPs and nurses participate in the same training courses as physicians, they can achieve similarly effective educational outcomes [12, 14]. Establishing new, separate courses specifically for NPs and nurses could be costly and may be unnecessary; instead, making existing physician-targeted courses more accessible to them is recommended. Given the clinical utility of POCUS training for NPs and nurses, the implementation of formal education programs for these practitioners is warranted [9,10,11, 13, 18].
Access to high-quality ultrasound machines was identified as the top facilitator, while NPs and nurses perceived the lack of such machines as a significantly greater barrier than did physicians. Limited access to ultrasound machines is a major issue not only in Japan but also in many other countries [4, 5, 7, 8, 20]. This problem is less pronounced in settings such as the intensive care unit, where ultrasound machines are readily available, but it remains a significant barrier in general wards and outpatient clinics [3]. Even for physicians, access to ultrasound machines can be challenging; thus, it is unsurprising that this issue poses an even greater barrier for NPs/nurses. Previous studies have also highlighted this concern [11].



留言 (0)