Central venous access is crucial in various scenarios and for multiple purposes, such as hemodynamic monitoring, administering medications with acidic or alkaline solutions (e.g., antibiotics), providing vasopressor support, or using hyperosmolar solutions via parenteral routes that exceed 800 mOsm/L [6, 7]. , however, CVCs have been associated with potentially fatal complications such as pneumothorax, bloodstream infections, and thrombosis [8]. Over the last 10 years, the practice of inserting PICCs has evolved, some evidence is controversial regarding complications related to PICC catheters versus CVCs, even so, it has been demonstrated that following good practices for inserting peripherally inserted central venous catheters reduces complications related to thrombotic events or CLASBI compared to central venous catheters [9]. Reports indicate a reduction in complications associated with central catheter insertion after implementing vascular access teams [10, 11]. In a survey designed to assess perceptions and decision-making patterns regarding vascular access in ICUs of 13 centers, it was found that evidence-based practices are followed inconsistently and vary according to the device, training status, ICU situation, and hospital size. Additionally, 59% of the centers did not have written guidelines or protocols on the appropriate type of vascular access for ICU patients. Likewise, having local vascular access guidelines and protocols was associated with improved adherence to certain evidence-based practices [12]. It has also been suggested that the use of PICC over CVC reduces costs for specialized vascular access equipment [13], highlighting the importance of generating institutional groups specialized in the insertion, follow-up, and active monitoring of vascular access. This aligns with our findings, and to our knowledge, our cohort is the largest related to an ultrasound-guided vascular access team trained from the ICU to support the entire hospital.
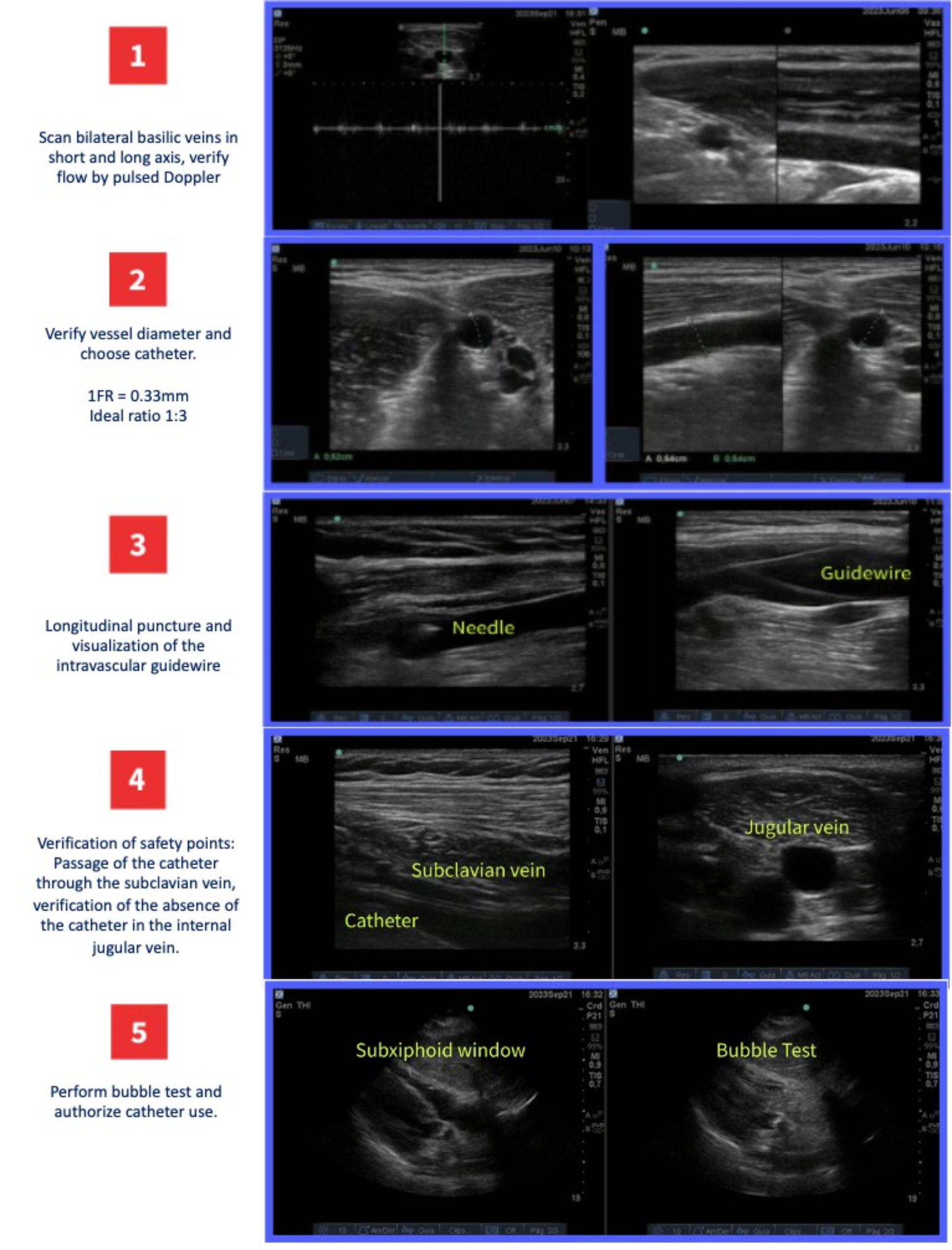
Our study shows a low incidence rate of PICC-related complications (CLABSI and CRT) and the risk factors related to these complications. Considering CRT, a meta-analysis aimed at identifying the incidence of thromboembolic events associated with the use of PICC in hospitalized patients, including those in the ICU, found an incidence of 3.7% of symptomatic deep vein thrombosis, with a higher incidence in critically ill patients (10.6%) [14]. CRT is associated with the catheter diameter ratio, the size of the catheter, and the location of the central line tip. A lower catheter-to-vein ratio and a smaller catheter diameter result in reduced impact on vein flow, decreasing the subsequent risk of thrombosis. In our practice, a catheter-to-vein ratio < 33% is encouraged (262 patients in our study surpassed that limit). In addition, implementing general ward and ICU protocols (Additional file 2: Fig. S2, Additional file 3: Fig. S3) to choose venous access devices might explain our findings. However, it should be noted that in our group, we do not actively search for asymptomatic thrombosis, which has been shown to have higher incidences in patients with PICCs, especially in superficial veins, particularly in the first 2 weeks after device insertion. It is also identified as a risk factor for CRT the low venous flow rates, which, as mentioned previously, is closely related to the catheter-vein ratio, and in most of our patients had a ratio of less than 1:3. We found no differences between left vs. right basilic vein puncture as a risk factor, which has been previously described as a risk factor for asymptomatic CRT (meta-analysis of asymptomatic DVT) [3]. Nevertheless, adherence to pharmacological antithrombotic prophylaxis could modify these results, the data of which are beyond the scope of this study. The adoption of evidence-based interventions, such as ultrasound-guided vein puncture [15], micro-introducers, novel materials, and sutureless securement devices [16] has also been shown to reduce PICC-related complications.
Regarding CLABSI previous evidence, a meta-analysis reported that patients with a PICC line have a lower CLABSI incidence (2.12 per 1000 catheter days) than those with CVCs (4.09 per 1000 catheter days), indicating a 48% lower risk of CLABSI in patients with PICCs [9]. We report similar incidence of CLABSI cases, most occurring in the ICU. Our findings might be attributed to daily follow-up strategies, which actively monitored all vascular accesses to identify early signs of local infection and constantly reassessed the catheter need.
The median number of catheter days was 10, which aligns with the Michigan Appropriateness Guide for Intravenous Catheters [17]. This guide recommends that PICC catheters should not be used in patients with a predicted duration of use below 6 days unless there are no other suitable vascular access options. Among the 605 patients with a PICC duration of less than 6 days, 72.9% were patients who were discharged, transferred to another institution, or died. The remaining patients required the PICC due to vesicant/irritant medications or parenteral nutritional administration or had limited vascular access.
The generalizability of these results is subject to certain limitations. For instance, the number of complications was low, which made unfeasible to perform a logistic regression model. Therefore, it is unknown if the identified risk factors are indeed risk factors or confounders, mediators, or effect modifiers. A longer study period or a multicentric study including a larger number of patients is required to perform multivariate analyses.
This study contributes to the safety profile evidence regarding the insertion and maintenance of PICCs. Following standard insertion guidelines, daily catheter routine care, and timely PICC removal should be implemented in institutions—particularly in ICUs—that regularly use PICCs to reduce the frequency of catheter changes and, most importantly, the number of catheter-related complications.




留言 (0)