
記住我



Patients who underwent RHC for various indications at Ramathibodi Hospital between September 2022 and July 2023 were consecutively screened. Patients aged ≥ 18 years who provided informed consent were included in the study. Patients who were pregnant, required mechanical ventilation, or if their IVC, HV, PV, IRV, or internal jugular vein (IJV) were unable to be identified, were excluded from the study. The study received ethical approval from the Institutional Review Board of the Faculty of Medicine Ramathibodi Hospital, Mahidol University (MURA2022/429).
Procedures and data collectionInclusion criteria included participants aged over 18 years, scheduled for RHC, and willing and able to provide informed consent. Exclusion criteria comprised individuals who were pregnant, unable, or unwilling to provide informed consent, and mechanically ventilated patients. Patient demographic information, medical history, and echocardiographic findings were collected from RAMAEMR if they met the inclusion criteria. The selection of data elements for chart analysis was a result of collaborative decision-making among all coauthors. One member of the research team, a medical resident in their 3rd year who possessed a strong command of medical terminology, conducted the data extraction process. The evening prior to RHC, the research staff conducted a telephone confirmation with the scheduled patients and, on the morning of the procedure, within a 4 h window prior to the scheduled time, the research staff approached the patients to acquire informed consent. Upon obtaining consent, the research staff proceeded with the VExUS protocol, IVC maximum diameter and its CI, uJVP. The ultrasonographers involved in this study included an internal medicine resident and an internal medicine attending physician. The internal medicine resident underwent comprehensive training in VExUS, IVC, and uJVP through a combination of online modules [19], and hands-on sessions by the internal medicine attending physician. The internal medicine attending physician, who is also one of the researchers in this study, is an expert in ultrasonography and has received specialized training in VExUS, IVC, and uJVP. We utilized inter-rater variability to assess agreement among the examiners. Additionally, a pulmonologist and a cardiologist were part of the research team, providing expertise in image assessment and confirming the accuracy of grading. It is important to note that the ultrasonographers and researchers were independent of the clinical team.
Blinding proceduresA member of the research team who performed the VExUS scans, IVC maximum diameter and its CI, and uJVP also participated in data entry, thus remaining unblinded to the results. However, the ultrasonographers documented the VExUS grading, IVC maximum diameter and its CI, and uJVP prior to the RHC procedure, and thus were blinded to the RAP data. Additionally, a clinician assessing RAP was blinded to VExUS grading, IVC maximum diameter and its CI and uJVP.
VExUS scanning and IVC maximum diameter and its CI protocolThe VExUS scan was performed using the Philips Lumify phased-array probe and the Kosmos Torso Probe from Echo Nous. Patients were positioned in a reclined position with the head of the bed elevated at a 30-degree angle. The ultrasonographer initiated the scan by measuring the diameter of the IVC using the sniff technique, recording both the maximum and minimum diameters. The CI of the IVC was then calculated using the formula: CI (Dmax—Dmin) / Dmax. Measurements were taken approximately 2 cm from the junction of the IVC and the right atrium, or 0–1 cm caudal to the confluence of the HV and the IVC. The HV waveform was evaluated by placing the probe either in a subxiphoid position (with the transducer positioned 1–2 cm below the xiphoid process and the probe marker directed towards 12 o'clock) or in a coronal view (with the transducer positioned at the junction of an imaginary line extending from the xiphoid process to the midaxillary line and the probe marker directed towards the patient’s right axilla). Pulsed wave Doppler waveforms were obtained by placing the sample volume within the HV, at least 1–2 cm away from the junction of the HV and the IVC. The PV waveform and its pulsatility were assessed in the same area as the HV, using a coronal view. The Pulsed wave Doppler gate was positioned across the PV, and the Doppler scale was lowered to increase the waveform amplitude. This adjustment increased the accuracy in calculating the PV pulsatility index. The formula used was: PV Pulsatility Index = (Vmax—Vmin) / Vmax. To visualize the IRV waveform, the probe was maneuvered caudally and posteriorly while maintaining its position relative to the HV and the PV. Using color Doppler, the imaging box was centered over the renal cortex or renal pyramid to reveal the intrarenal vessels. The Pulsed wave Doppler gate was then positioned on the interlobar vessels to observe the waveform of the IRV [17].
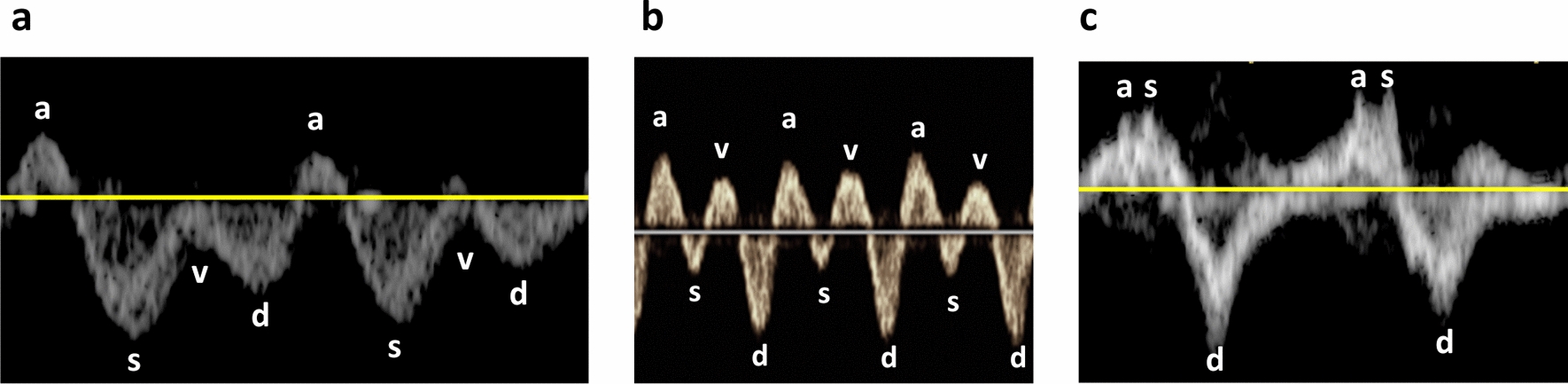
The VExUS comprises evaluations of pulsed wave Doppler of HV, PV, and IRV. HV: Normal HV Doppler waveforms exhibit a small retrograde a-wave, followed by anterograde S and D waves, with the S wave being deeper than the D wave (Fig. 1a). In mildly abnormal HV waveforms, the S wave is less deep than the D wave (Fig. 1b). Severely abnormal HV waveforms show a reversal of the S wave, with only the D wave as a negative deflection wave (Fig. 1c). PV: A normal PV Doppler waveform demonstrates minimal pulsatility, with a pulsatility index < 30% (Fig. 2a). A pulsatility index of 30–49% is considered mildly abnormal (Fig. 2b), while a pulsatility index > 50% is classified as severely abnormal (Fig. 2c). IRV: A normal intrarenal Doppler pattern exhibits arterial pulsations generating a regular positive deflection wave, and IRV generating a continuous, smooth negative deflection wave (Fig. 3a). As renal venous congestion increases, venous pulsations become visible. In mildly abnormal waveforms, venous pulsations with clearly visible anterograde S and D waves are present (Fig. 3b). Severely abnormal waveforms display a retrograde S wave with only an anterograde D wave [17] (Fig. 3c).
Fig. 1
a Normal HV Doppler waveforms exhibit a small retrograde a-wave, followed by anterograde S and D waves, with the S wave being deeper than the D wave. b In mildly abnormal HV waveforms, the S wave is less deep than the D wave. c Severely abnormal HV waveforms show a reversal of the S wave, with only the D wave as a negative deflection wave; HV Hepatic Vein
Fig. 2
a A normal PV Doppler waveform demonstrates minimal pulsatility, with a pulsatility index < 30%. b A pulsatility index of 30–49% is considered mildly abnormal, c while a pulsatility index > 50% is classified as severely abnormal; PV = Portal Vein
Fig. 3
a A normal intrarenal Doppler pattern exhibits arterial pulsations generating a regular positive deflection wave, and IRV generating a continuous, smooth negative deflection wave. As renal venous congestion increases, venous pulsations become visible. b In mildly abnormal waveforms, venous pulsations with clearly visible anterograde S and D waves are present. c Severely abnormal waveforms display a retrograde S wave with only an anterograde D wave; IRA Interlobar Renal Artery, IRV Interlobar Renal Vein
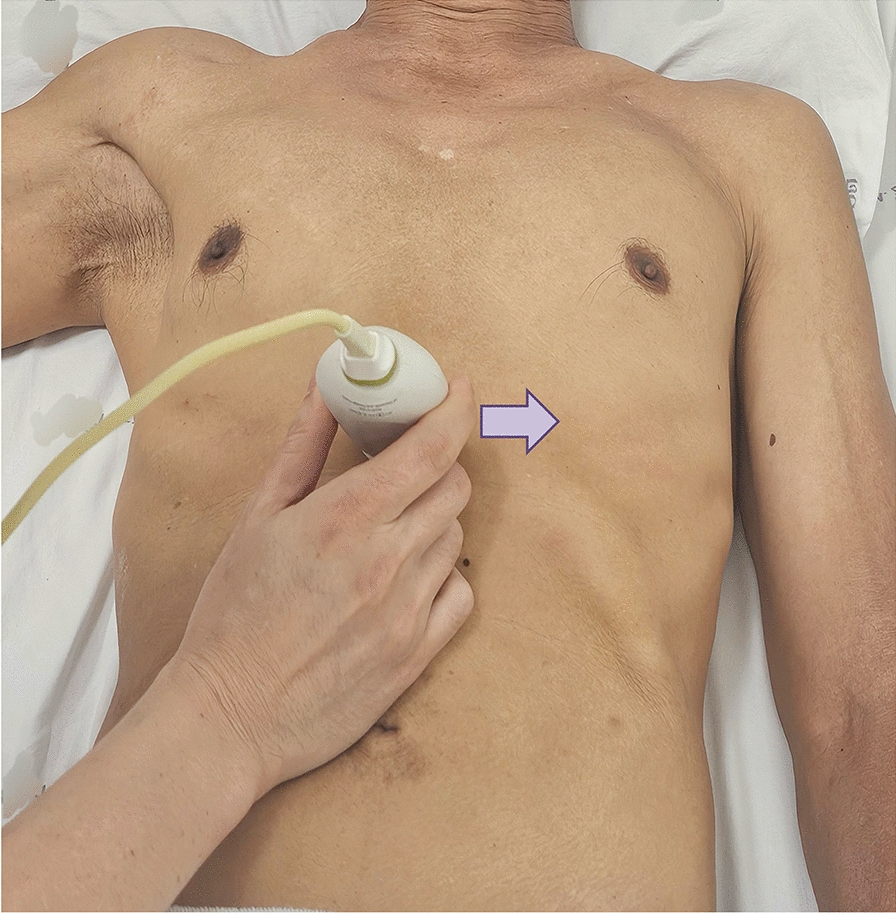
uJVP protocolThe uJVP was performed using the Philips Lumify ultrasound system with a high-frequency probe. Patients were positioned in a reclined position with the head of the bed elevated at 45 degrees. The ultrasound probe was initially placed between the two heads of the sternocleidomastoid muscle, with the probe marker pointing towards the patient's right side. In the transverse view, the internal jugular vein could be visualized alongside the common carotid artery (Fig. 4). If the internal jugular vein was not clearly visible and appeared collapsed at this position, the head of the bed was adjusted to a lower angle of around 15–30 degrees, and the visualization was rechecked. The probe was then slid cephaladly until the internal jugular vein collapsed, and the probe marker was rotated to point towards the patient's head. The goal was to locate the neck bottle sign, which indicated the point of collapse in the internal jugular vein (Fig. 5). This area was marked on the patient’s neck, and the jugular venous pressure was measured by determining the height from this point to the sternal angle in centimeters of H2O. To obtain the actual jugular venous pressure, 5 cm was added to this measured distance [14].
Fig. 4
In the transverse view, the IJV can be visualized alongside the CCA; IJV Internal Jugular Vein. CCA Common Carotid Artery
Fig. 5
The neck bottle sign, which indicates the point of collapse in the IJV (arrow); IJV Internal Jugular Vein, CCA Common Carotid Artery
Conventional VExUS grading system (VExUS)VExUS grade 0 is assigned when the maximum IVC diameter is ≤ 2 cm. VExUS grade 1 is assigned when the maximum IVC diameter is > 2 cm and there is a combination of normal or mildly abnormal waveforms without any severely abnormal waveforms in HV, PV, and IRV. VExUS grade 2 is given when the maximum IVC diameter is > 2 cm and there is one severely abnormal waveform in either HV, PV, or IRV. VExUS grade 3 is assigned when the maximum IVC diameter is > 2 cm and there is ≥ 2 severely abnormal waveforms in HV, PV, or IRV [17].
Newly introduced modified VExUS grading system (mVExUS)In our newly introduced mVExUS classification system, mVExUS Grade 0 is assigned when the maximum IVC diameter is < 2 cm with CI of ≥ 50%; mVExUS Grade 1 is designated for cases where the maximum IVC diameter is < 2 cm and CI is < 50% or the maximum IVC diameter is ≥ 2 cm and CI is ≥ 50% and there is a combination of normal or mildly abnormal waveforms without any severely abnormal waveforms in HV, PV, or IRV; mVExUS Grade 2 is given when the maximum IVC diameter is < 2 cm and CI is < 50% or the maximum IVC diameter is ≥ 2 cm and CI is ≥ 50% and there is one severely abnormal waveform in either HV, PV, or IRV; and mVExUS Grade 3 is assigned when the maximum IVC diameter is < 2 cm and CI is < 50% or the maximum IVC diameter is ≥ 2 cm and CI is ≥ 50% and there are two or more severely abnormal waveforms in HV, PV, or IRV.
IVC classification by American society of echocardiographyThe American Society of Echocardiography classifies the IVC into three groups: Class 1 is designated when the maximum diameter of these IVC is ≤ 2.1 cm with CI ≥ 50%. Class 2 is assigned when the maximum diameter of the IVC is ≤ 2.1 cm with CI < 50%, or when the maximum diameter of the IVC is > 2.1 cm with CI ≥ 50%. Class 3 is allocated when the maximum diameter of the IVC is > 2.1 cm with CI < 50% [12].
Right heart catheterizationPatients underwent RHC within 4 h of the ultrasound examination, performed by a cardiologist staff member with expertise in RHC, who subsequently recorded the RAP during the RHC procedure. We employed a 6 or 7-French balloon flotation catheter, inserted via the femoral or jugular venous approach, to measure the RAP while the patient was in the supine position. For patients in sinus rhythm, the mean of the 'a' wave during end-expiration was utilized. Conversely, the pressure at the end of the QRS complex was used to represent the RAP in other cases. Importantly, the clinician who conducted the RHC was blinded to the VExUS grading, IVC diameter, CI, and uJVP measurements.
Statistical analysisContinuous variables were summarized as mean with standard deviation (SD) or median with interquartile range, depending on the normality of the data, which was assessed using the Shapiro–Wilk test. Categorical variables were presented as frequency and percentage. To compare the median RAP across ASE classification or VExUS grade, Kruskal–Wallis test was performed with pairwise comparison adjusted by the Bonferroni correction for multiple tests. In assessing inter-rater variability, Cohen’s kappa statistic was employed to compute the agreement among the raters for each variable. Spearman’s correlation coefficient was calculated to assess the correlation between RAP and uJVP, and the Bland–Altman method was employed to visually evaluate their agreement. Statistical analysis was performed using Stata, version 18.0 (StataCorp).
留言 (0)