
記住我



VExUS is often referred to as a tool to quantify a patient’s volume status. Firstly, we would like to discourage the use of the term volume status, which is an exceedingly vague concept that is often understood differently by different physicians. For example when someone uses the term volume status, it is unclear whether they are referring to intravascular volume, both intra-and extravascular volume, stressed or unstressed volume, etc. There has been a longtime love affair with the somewhat quixotic quest for a “fuel gauge” of intravascular volume which started with the central venous pressure (CVP), then the superior and inferior vena cava (SVC/IVC), and now, in many clinicians’ minds, the VExUS score. This exposes a certain misunderstanding or hopeful attempt to shortcut the non-linear relationship that exists between volume and pressure. While they are obviously related, in a multi-compartmented system with varying elastances, it is simply impossible to use pressure as a measure for volume - or vice-versa: it is time for clinicians to let go of this dream. All the above failed as simple gauges of “volume status”, through no fault of their own, but rather because the question asked was an impossible one.
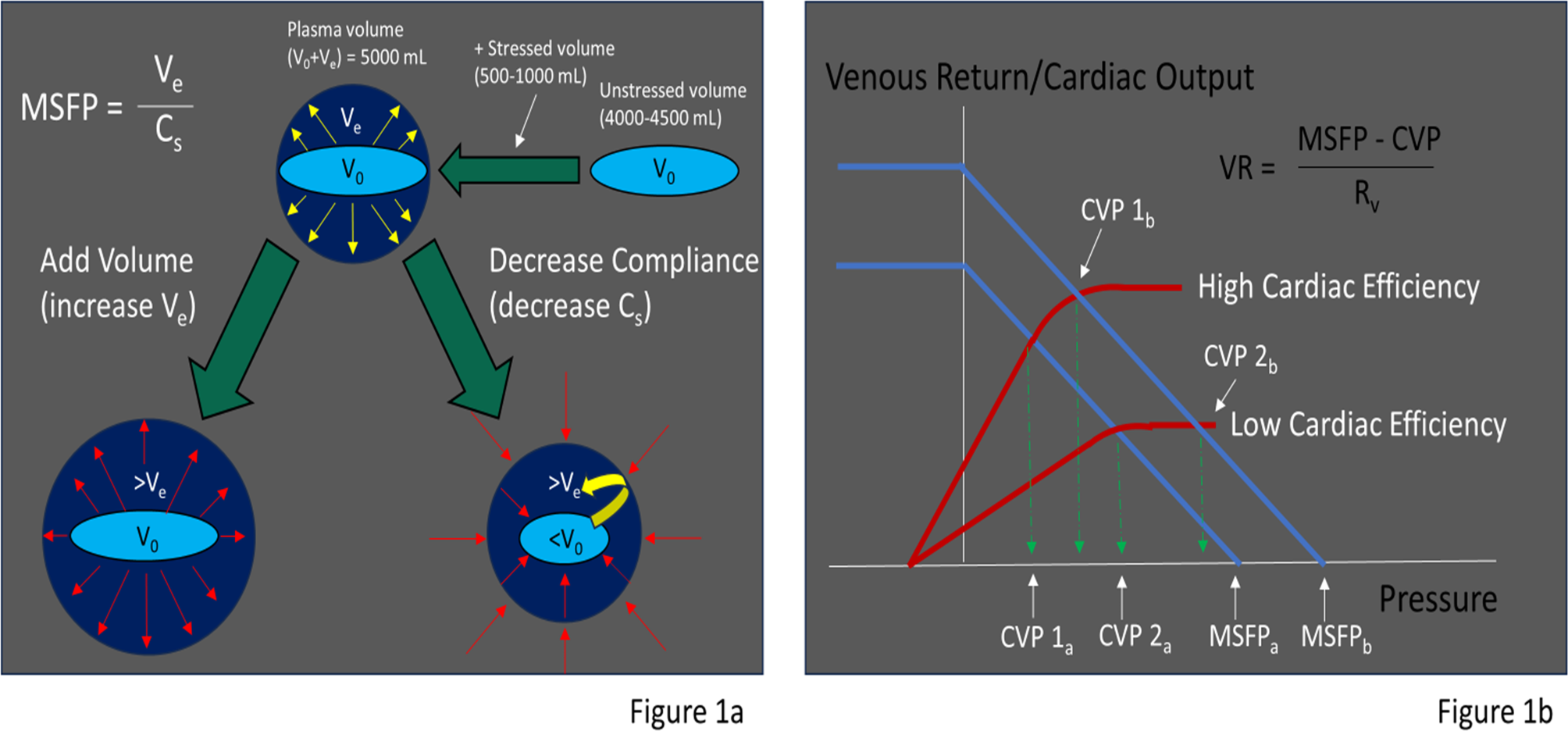
So, what does VExUS truly measure? It reflects the ever changing relationship between the upstream venous pressure (mean systemic filling pressure (MSFP) and right atrial pressure. The MSFP, crucially, depends on two distinct factors that interact to determine this pressure. Firstly, there is the volume that “stretches” the walls of the collective blood vessels leading to elastic recoil creating pressure (as opposed to unstressed volume which is considerable, but does not distend the highly compliant venules), and secondly there is the degree of compliance in the blood vessels. The less compliant the blood vessels, the more a stressed volume will generate a pressure. The CVP depends on the magnitude of the MSFP and the efficiency of the right ventricle (RV), which when working well will keep the CVP low. The venous return (VR)--which equals the cardiac output in the steady state–depends on the difference between the MSFP and the CVP. (Figure 1a and b)
Fig. 1
1a: Intravascular volume is composed of unstressed volume that does not distend the vascular walls and stressed volume that distends the walls resulting in elastic recoil of the walls generating the MSFP. MSFP increases with increased stressed volume (where the walls are further distended) and decreased compliance (where the vessels become stiffer and unstressed volume is converted to stressed volume). 1b: The CVP depends on the cardiac efficiency and the MSFP. Venous return is driven by the difference in MSFP and the CVP. When CVP = MSFP venous return will be zero. Increases in the MSFP or decreases in the cardiac efficiency will increase CVP, but the CVP and cardiac output depends on the operating point where the venous return line and Frank-Starling curves intersect. V0= unstressed volume, Ve=stressed volume, Cs=systemic vascular compliance, Vr=resistance to venous return, VR= Venous Return
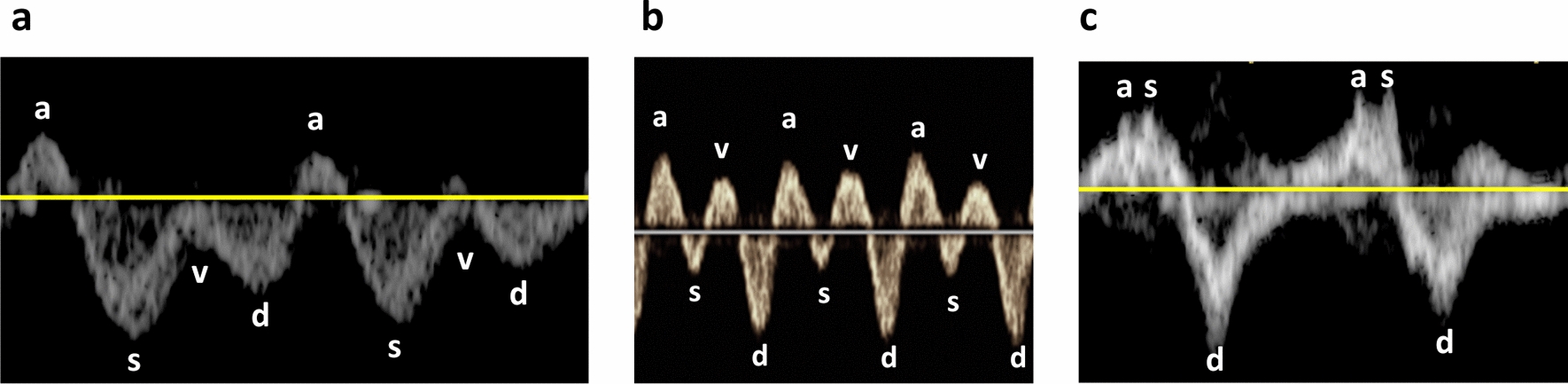
In a patient who is initially normovolemic but infused with enough fluids, we will observe a rise in their MSFP which in turn will lead to a rise in CVP. If continued, this indiscriminate fluid administration will increase preload until the right ventricle is anatomically incapable of accommodating further volume expansion, and CVP will start to rise sharply [3]. (Fig. 2a) The venous system–having a large capacitance–is forgiving to a point. This point is the limit of venous compliance, where PMSF will then quickly rise, preserving VR at the expense of pathologically increased capillary hydrostatic pressures. (Fig. 2b) This will eventually result in a plethoric IVC and transmission of pressure waves upstream, causing abnormal Doppler envelope changes and an elevated VExUS score. In such a case, VExUS will correlate to intravascular volume.
Fig. 2
2a: A normovolemic person is infused with repeated boluses of crystalloid, thus raising the MSFP. Initially the response is to increase the VR with only small increases in the CVP. However, once the limit of RV compliance is reached the CVP and MSFP rapidly rise with little increase in VR. The rise in MSFP results in venous congestion of the organs and limits perfusion. 2b: Relationship of venous compliance. Initially, additional stressed volume raises the venous pressures minimally until the limits of compliance is reached. At that point the venous pressures rapidly rise with addition of even small amounts of volume
Now take for example a patient who develops a large pulmonary embolism, leading to a acute increase in pulmonary arterial pressure and marked right ventricular failure, the CVP will rise due to the inability of the RV to handle its afterload, and, if sufficiently elevated, will result in increasing VExUS scores. Without an additional rise in intravascular volume. (Fig. 3)
Fig. 3
An acute rise in RV afterload due to a pulmonary embolism causes a significant decrease in RV efficiency. The VR drops whilst the CVP rises. Any attempt at a volume challenge will most likely result in an increase in the CVP and MSFP without a significant increase in the VR
In a third potential scenario, a patient presents with septic shock. Here, the vasodilation will lead to a decrease in MSFP and thus venous return, with an inevitable drop in CVP. This would decrease IVC size and - if congestion had been present, VExUS score. No change in intravascular volume once again. (Fig. 4) Conversely, as this patient improves, resolving vasoplegia will increase MSFP and thus venous return and congestive indices may appear, also without a change in intravascular volume. Septic shock and RV failure can of course co-exist, with the resulting VExUS score reflecting a balance between the degree of vasodilatation and RV failure.
Fig. 4
An acute rise in systemic vascular compliance (without a change in volume) results in a decrease in MSFP, CVP, and VR. Administration of either a vasopressor or a crystalloid bolus will shift the MSFP toward normal. However, note that the original drop in MSFP was independent of actual volume, and was instead a result of a change in vascular compliance alone
So, for instance, following the stable outpatient with congestive heart failure (CHF) and no other active process, a change in VExUS score is likely to reflect a change in the intravascular volume and perhaps extracellular water. In support of this, Husain-Syed et al. showed a correlation between overhydration determined by bioimpedance analysis and worsening intra-renal venous Doppler patterns in a cohort of non-critically ill right heart failure patients [4].
So can the VExUS score be used to assess intravascular volume at all? Yes, but only in the same patient without change in vascular compliance or RV-PA coupling (i.e. a decrease in RV efficiency). In the critically ill patient? Not really. With regard to VExUS, intravascular volume is one part of a comprehensive interlinked system.
留言 (0)