The main aim of the present study was to determine the changes in cardiac, muscular and renal biomarkers in healthy overweight or adults with obesity subjected to prolonged aerobic exercise through participation in a half-marathon, a 30-km run or a marathon based on the different cardiorespiratory fitness and performance levels they achieved at the end of the 24-week training programme (D’Alleva et al. 2023).
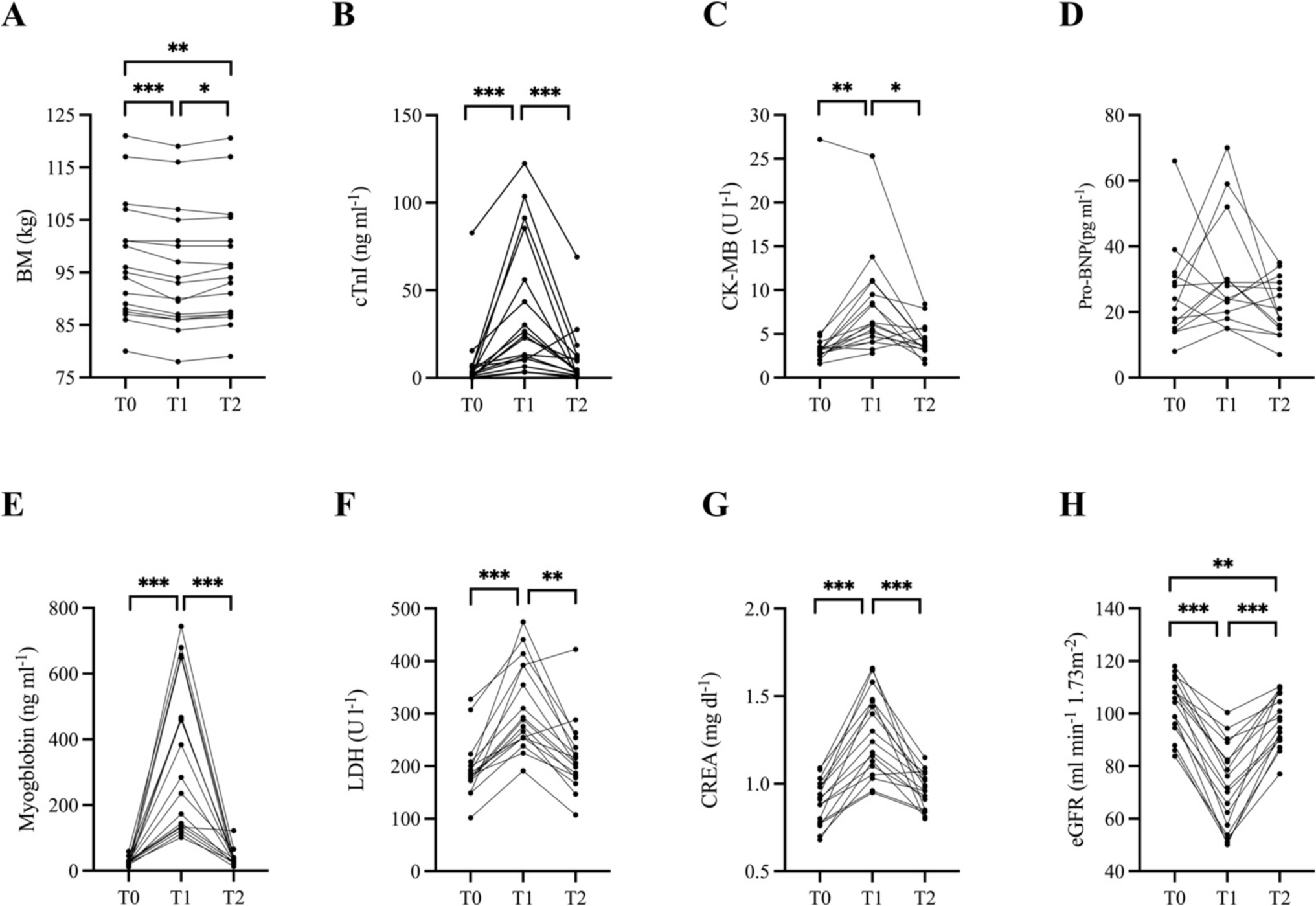
The main findings induced by running competition were (1) a significant reduction in BM not fully recovered 72 h after the race and a significant increase in the circulating levels of cTnI, CK-MB, myoglobin, LDH, CREA and eGFR, which returned to the reference limits 72 h after training; (2) ∆cTnI was correlated with the FFM baseline values; (3) ∆CK-MB was correlated with running-related variables; (4) ∆myoglobin was correlated with the baseline values of V’O2GET, velocity corresponding to ventilatory thresholds and V’O2max, and running-related variables; and (5) ∆CREA and ∆eGFR were correlated with training parameters.
In our study, we observed a transient increase in cardiac biomarkers (i.e. cTnI and CK-MB) after prolonged exercise. However, Pro-BNP increased after the marathon, albeit not significantly, similar to the results shown by Hu et al. (2023) in amateur runners. Instead, Traiperm et al. (2021), Sierra et al. (2019) and Hottenrott et al. (2016) reported a large increase in NT-Pro-BNP values after a marathon in elite and nonelite runners, which returned close to baseline 24 h after the race in all runners. However, despite the high NT-proBNP increase, no traumatic structural damage to the myocardium was detected by magnetic resonance (Traiperm et al. 2021).
The cTn is the most frequently measured cardiac marker for assessing the effects of prolonged exercise, and the majority of studies have shown an increase in cTnI after half-marathon, marathon or ultramarathon races in normal-weight subjects with different grades of training, as described in a recent meta-analysis (Rubio-Arias et al. 2021). In our study, post-race cTn levels increased successively after the race but returned to baseline 72 h after the race, which is in agreement with the findings of most studies in recreational athletes (e.g., a mean age of 38.6 years and a mean marathon time of 03 h and 30 min), who reported cTn levels in the reference value range within 96 h post-race (Bernat-Adell et al. 2019; Sierra et al. 2019). CK-MB followed the same trend as cTnI, increasing after the competition and then gradually decreasing until returning to initial values after 72 h post-race. These findings are in agreement with the findings of Hottenrott et al. (2016) in recreational athletes; however, CK-MB remained altered in recreational athletes even 15 days after the race in the study by Sierra et al. (2019). When we compare our data with those of studies conducted in recreational and well-trained runners during marathon and ultramarathon races on uphill, downhill or mixed terrain, we find similar values for the increase in markers of cardiac damage (e.g., cTnI, CK-MB and NT-Pro-BNP), which were six to ten times greater after the race (Koller et al. 2008; Da Ponte et al. 2018; Giovanelli et al. 2020). Therefore, the transient increase in cardiac damage biomarkers after prolonged exercise might be multifactorial. First, the response to extreme exercise in recreational and well-trained athletes could depend on genetic factors (Sierra et al. 2019) and nutritional status (Mielgo-Ayuso et al. 2020). However, genetic factors may not be the only players in this context. Indeed, the meta-regression of Rubio-Arias et al. (2021) reported a negative interaction between cTnI levels after a marathon and BMI in subjects with normal weight. Similarly, Shave et al. (2007) reported that in long-term aerobic events, the amount of cTnT released was related to BM. Nevertheless, Eijsvogels et al. (2012) reported that after a 30-, 40- and 50-km walk, the magnitude of absolute cTnI increase was comparable among lean, overweight, and individuals with obesity, suggesting that exercise intensity (i.e. as a percentage of HRMAX), rather than anthropometric factors, was the most important predictor of cTnI release after a long endurance event. In the present study, no relationship was observed between the ∆cTnI values and the baseline BM and FM. Nonetheless, a positive correlation was observed between ∆cTnI and baseline FFM, suggesting that cardiac work is greater in those with greater muscle mass. However, this finding should be confirmed in future studies. In addition, other studies have reported that the release of cTnI after long endurance events is influenced by other factors, such as exercise duration (Eijsvogels et al. 2015), energy expenditure during the race (Bernat-Adell et al. 2019) and training intensity [e.g., expressed as the mean HR, HR as a percentage of HRMAX and HRRCP (%) and marathon velocity expressed as VRCP (%)] (Martínez-Navarro et al. 2020b; Rubio-Arias et al. 2021)]. In this study, we did not observe a correlation between ∆cTnI and running-related variables, as previously reported by Da Ponte et al. (2018).
With respect to CK-MB, the ∆CK-MB induced by the race was positive and significantly correlated with the time spent in Zone 3 (%) during training and displayed a trend towards significance when assessing its correlation with training time and luTRIMPHR. The latter suggests that the sustained increase in cardiac output over several hours of aerobic exercise, especially the time spent at high intensity, contributed to an increase in the myocardial workload, leading to the cytosolic release of biomarkers without true damage to myocytes (Hewing et al. 2015; Janssen et al. 2023).
In line with previous studies in experienced amateur runners, the present findings support the notion that prolonged aerobic exercise (i.e. over 90 min duration) also caused a transient increase in serum biomarkers of muscle damage (i.e. myoglobin and LDH) (Hottenrott et al. 2016; Del Coso et al. 2017), which returned to baseline levels within 72 h after the race. In addition, LDH levels increased after races within the marathon distance by an average of ~ 111 to – 129 U l−1 (e.g., similar to our results) (Shin et al. 2016; Bernat-Adell et al. 2019), started to decrease 48 h after the race (Arakawa et al. 2016) and reached normalization 8 days after the race (Bernat-Adell et al. 2019). Instead, in the present study, LDH levels returned to baseline values within 72 h after the race compared with those reported in recreational participants in previous studies (Shin et al. 2016; Bernat-Adell et al. 2019). Several studies have shown that the release of myoglobin and LDH after long endurance competitions depends on the competition time (Bernat-Adell et al. 2019), running surface (e.g., uphill and downhill) (Giandolini et al. 2016; Da Ponte et al. 2018; Giovanelli et al. 2020), energy expenditure during the competition (Bernat-Adell et al. 2019), running intensity during the events (Hottenrott et al. 2016), heat and humidity (Gutiérrez-Vargas et al. 2018), and exercise-associated muscle cramps (Martínez-Navarro et al. 2020a). Compared with our results, we observed a similar increase in LDH after prolonged aerobic exercise in all the above conditions, whereas the increase in myoglobin was lower in our case than in running races with different surfaces. The latter could be partly due to the fact that compared to running on flat surfaces, running on uphill and downhill surfaces involves more work for type I and type II muscle fibres (Gottschall and Kram 2005), as concentric (e.g., uphill) (Gottschall and Kram 2005) (Gottschall and Kram 2005) and eccentric (e.g., downhill) (Giandolini et al. 2016) muscle contraction is more pronounced.
In the present study, no correlations between LDH and baseline anthropometric data, physical capacity, or running-related variables were detected. In contrast, ∆myoglobin levels were moderately correlated with baseline physiological parameters (i.e. V’O2GET, VMAX, VRCP and VGET) and running-related variables [e.g., marathon time, luTRIMPHR, mean HRGET (%), and mean marathon speed (km h−1)] and strongly positively correlated with time spent in Zone 3 (%) during the marathon. It is possible that a longer race time and greater average running intensity, despite different running distances, increase skeletal muscle damage and consequently increase the circulating levels of damage-related biomarkers after prolonged aerobic running (Gutiérrez-Vargas et al. 2018). In addition, muscular pH may decrease after a marathon, leading to fatigue with a decrease in force generation capacity, passive muscle tension and stiffness (Metzger and Moss 1990). To our knowledge, this is one of the first studies to compare biomarkers of muscular damage after long-term training and running-related parameters such as training load calculation (i.e. with luTRIMPHR) and the time spent in the three different HR zones during training in a cohort of participants with overweight or obesity.
Third, the transient increase in CREA levels and concomitant decrease in eGFR after prolonged aerobic exercise were observed as part of this study (i.e. over 90 min in duration), which suggested the onset of acute kidney injury in 35% of participants (Mehta et al. 2007; Shin et al. 2016). Previous studies have shown that serum CREA concentrations increase significantly by ~ 0.19–0.21 mg dL−1 after marathon and ultramarathon races in normal-weight recreational and well-trained athletes when different surfaces (e.g., uphill and downhill) are considered (Hewing et al. 2015; Poussel et al. 2020). In our study, the mean CREA increase was ~ 0.39 mg dL−1, and these differences could be due to the higher BMI of our participants. In addition, CREA levels returned to baseline within 72 h of the race and were within the reference range, which is consistent with previous studies in recreational and well-trained runners (Hewing et al. 2015; Poussel et al. 2020). For eGFR, previous studies in recreational and well-trained runners have shown that eGFR decreases after long-distance running (Hewing et al. 2015; Poussel et al. 2020) and returned to baseline at 24 h after the race (Panizo González et al. 2019). Instead, in this study, eGFR was lower even at 72 h post-race versus pre-race levels. This finding may be partly explained by the late arrival of intracellular toxic waste in the kidney, which was confirmed by the altered myoglobin and LDH levels, which were above the URL in 5.9% and 21.4% of participants, respectively (Panizo González et al. 2019). The physiological factors that contribute to the transient increase in renal biomarkers after prolonged exercise are multiple and contrasting. A few available studies in recreational and well-trained runners have shown that both the duration of the race and the main intensity of the race during a marathon or ultramarathon are more likely to lead to kidney damage (McCullough et al. 2011; Shin et al. 2016), whereas Hewing et al. (2015) reported a weak but significant negative correlation between lower eGFR values and the duration of the race. In addition to distance, some authors report an increase in markers of acute kidney damage after a marathon or ultramarathon on uphill, downhill or mixed terrain (Da Ponte et al. 2018; Giovanelli et al. 2020) due to increased concentric and eccentric muscle load and dehydration (Rojas-Valverde et al. 2021). However, there are conflicting results concerning the relationship between dehydration status and skeletal muscle damage after long-distance running with acute kidney injury (McCullough et al. 2011; Panizo González et al. 2019; Poussel et al. 2020).
In this study, no correlation was found between ∆CREA or ∆eGFR and baseline anthropometric data and physical capacity. Rather, ∆CREA values were moderately correlated with running-related variables (e.g., luTRIMPHR, mean HR of the race as a percentage of ventilatory thresholds and V’O2max) and strongly correlated with training time spent in Zone 3 (%). We also observed a negative correlation between the decrease in eGFR after a training session and the training time of participants in Zone 3 (%). It is possible that the higher average training intensity despite different training distances or training times (i.e. as shown by the negative correlation between CREA and race time in Zone 1) contributed to transient muscle damage that may lead to renal dysfunction due to glomerulus degeneration and reduced renal blood flow, resulting in reduced oxygen and energy supply and thus ischaemic damage to vascular endothelial cells (Brezis and Rosen 1995). Further studies are needed to better understand the mechanisms of acute kidney injury after long-distance running and to characterize the molecular mechanisms involved.
The present study has several limitations. First, although we detected changes in cardiac, muscular and renal biomarkers after prolonged aerobics, we did not consider a pre-exercise diet; food consumed during exercise; or hydration status before, during and after exercise. Although we measure the BM before and after the race, we do not know whether additional nutritional factors and hydration status could influence the results obtained. Second, although we observed a transient increase in markers of heart, muscle and kidney damage after exercise, we do not know if the affected organs were damaged. Future studies will also have to consider this last aspect. Third, our study involved a small sample size of healthy overweight or adults with obesity having different training levels (D’Alleva et al. 2023), and it was not possible to distinguish between the effects of the 3 different race distances (i.e. half-marathon, 30-km and marathon) on cardiac, muscular and renal biomarkers. Future studies are needed to further explore these aspects.
In conclusion, the results of this study provide a comprehensive overview of how cardiac, muscular, and renal damage occurs following prolonged running and 72 h post-exercise in a cohort of healthy adults with overweight or obesity. This is particularly important, as the number of recreational athletes, especially with overweight or Grade I obesity, competing in half-marathons or marathons has increased over the last 10 years. Therefore, when planning athletes' pre- and post-race training sessions, coaches should carefully consider the impact of baseline anthropometric data, physical capacity and running-related variables on markers of cardiac, muscular and renal damage.

留言 (0)