Study design
We conducted a prospective observational cohort study at our tertiary referral center in France, including all consecutive patients referred to our center for the endoscopic resection of a colorectal neoplasia > 2 cm, between January 2019 and January 2020.
Patients aged of ≥ 18 years old without previous history of endoscopic resection nor resection attempt were included. Information on lesion characteristics, such as biopsies or images from previous endoscopy reports, was not provided to the physician in charge of endoscopic characterization and resection.
Patients were excluded in case of underlying inflammatory bowel disease, or when the specimen was not resected en bloc R0 in case of adenocarcinoma. When ESD was not curative and the histological analysis reported deep invasive adenocarcinoma, the patient was included considering that the histological analysis could not be underestimated. In case of focal positive horizontal margin with only SSL (Sessile Serrated Lesion) or low-grade dysplasia, the lesion was not excluded considering that the histological analysis was of good quality without loss of information.
The Ethics Committee of Hospices Civils de Lyon approved the study, and all patients gave informed consent before their procedures. The study was declared on the national clinical trial register with the number NCT04482491.
Colonoscopy procedures
All colonoscopies were performed by three senior endoscopists (M.P., J.R., F.R.), experienced in advanced diagnosis and ESD (over 300 procedures each) with the patient under general anesthesia and using CO2 insufflation. Optical characterization of lesions was performed using high-definition white light endoscopy followed by close-up examination assisted by virtual chromoendoscopy, with or without magnification, using Olympus CF-HQ190 L/I colonoscopes (Olympus, Tokyo, Japan).
Resection techniques used to obtain high-quality histological assessment
In this study, to avoid missing information, we aimed to obtain for all colorectal neoplasia > 2 cm included a high-quality histological assessment [7]:
For lesions without any suspicion of deep invasive component (lesions > 2 cm without any suspicion of deep invasive component and lesions with a tiny area < 5 mm of amorphous pit or vascular patterns as proposed by Japanese guidelines [12]), an ESD was performed with an en bloc R0 intent.
For lesions with high suspicion of deep invasive component (lesions with a large amorphous area > 5 mm), a surgery was performed after the following endoscopic biopsy protocol to achieve a surgical R0 resection with lymphadenectomy.
Biopsy procedures
When ESD was feasible, biopsies were performed after the end of the procedure, on the specimen itself after stretching it on cork, to avoid any damage or bleeding that could have interfered with the resection leading to an over risk for the patient. If an area appeared suspicious of focal invasion during endoscopic characterization, a targeted biopsy (TB) was done on this area, after recognition of the area on the specimen itself, guided with the endoscope using white light imaging (WLI) and/or virtual chromoendoscopy. A non-targeted biopsy (NTB) was then randomly performed anywhere in the lesion. In the case when no area was suspicious of invasion, only a single NTB was performed.
When a surgical resection was proposed, TB and NTB were performed in the same way, directly after endoscopic characterization in the colon or rectum.
Histological examination
Histopathological examination was carried out by two different expert digestive pathologists, double blinded from the result of the other analysis and the endoscopic prediction, according to the Vienna [13] and TNM [14] classifications. For biopsies specimen, as depth of invasion could not be estimated, an “infiltrating aspect” was considered as deep invasive adenocarcinoma.
Study primary objective
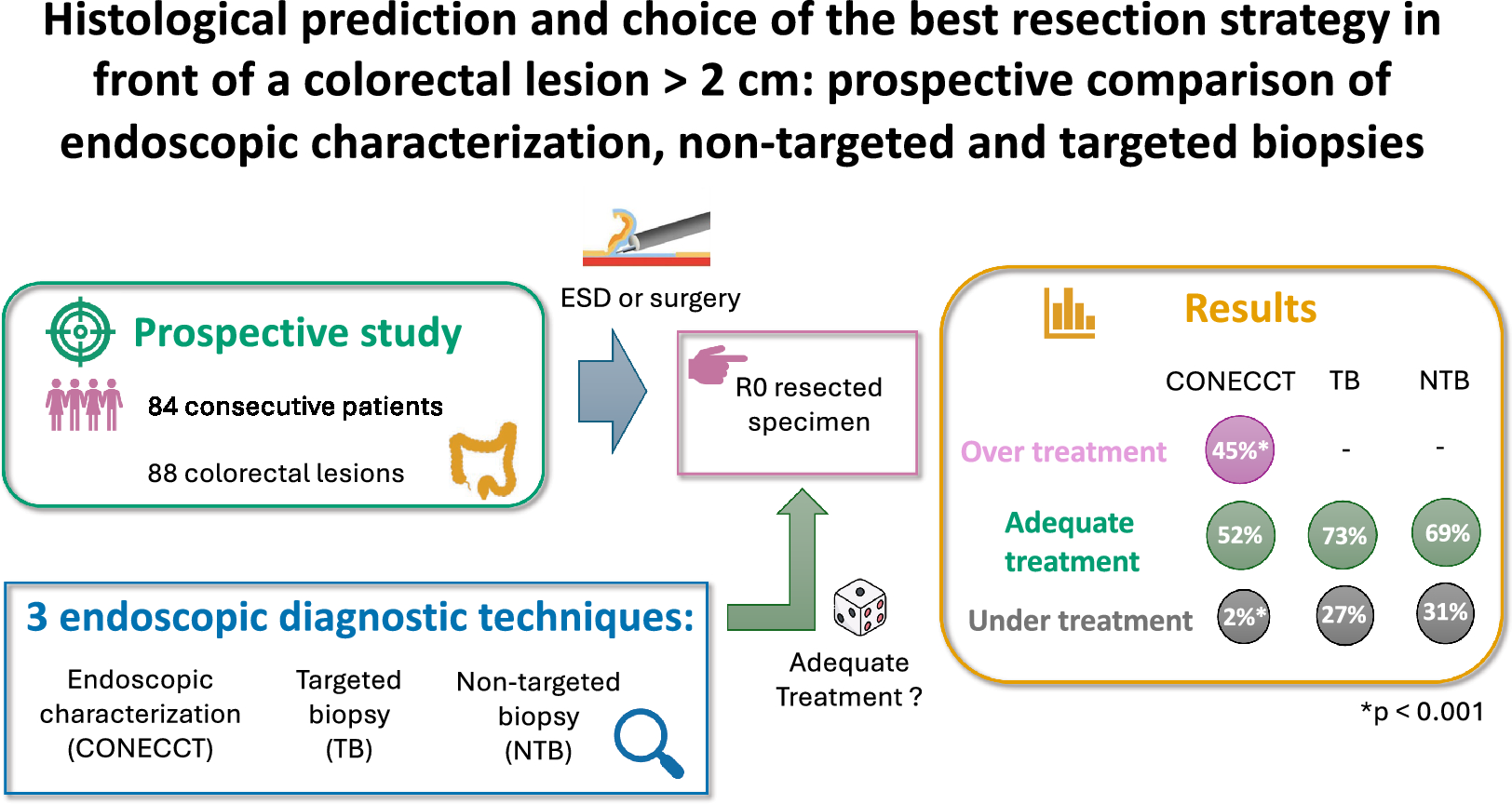
The primary objective was the evaluation of the best strategy between endoscopic characterization and targeted or non-targeted biopsies, so that the proposed resection technique offered a level of quality of tumor resection adapted to the definitive histology of the lesion on resected specimen, defined by the following:
Resection without R0 intent (piece meal) for sessile serrated lesion (SSL), low-grade (LGD) and high-grade (HGD) dysplastic adenoma (CONECCT IS or IIA, Kudo II, III or IV, Sano I or II),
En Bloc R0 resection (ESD) for intramucosal adenocarcinoma, superficial submucosal adenocarcinoma with < 1000 μm submucosal invasion (CONECCT IIC, Kudo Vi, Sano IIIA),
Surgical resection with R0 intent for deep invasive lesions: deep submucosal adenocarcinoma with > 1000 μm submucosal invasion, intramuscular or deeper T2-T3 cancer (CONECCT III, Kudo Vn, Sano IIIB, infiltrating aspect without any precision at the histology report of biopsies).
“Adequate treatment” was defined when the proposed resection technique offered a level of quality of tumor resection adapted to the definitive histology of the lesion, “under treatment” when it led to an insufficient level of quality of tumor resection and “over treatment” when an overly invasive resection technique would have been proposed.
Study secondary objectives
Secondary objectives were the diagnostic accuracy to predict histology (sensitivity Se and specificity Sp) of endoscopic characterization, TB and NTB, the evaluation of adequacy of proposed treatment by biopsies with final histology if we consider that the presence of cancer whatever its depth would lead to surgical treatment, and adverse events occurring during or after endoscopic and surgical resections.
Data collection
The data collected were patient demographics including sex and age at the time of colonoscopy; lesion characteristics: location, size, morphology, classification according to Paris, Kudo, Sano, and CONECCT classifications, histology of TB, NTB and final histology after ESD or surgical resection.
Statistical analysis
Continuous variables were presented as mean ± standard deviation or median with the first and the third quartile. Categorical variables were presented as numbers and percentages. A chi-square test was used to compare adequacy of proposed treatment with final histology. Diagnostic accuracy was assessed by sensitivity and specificity. A Mc Nemar test was used to compare sensitivity and specificity between paired groups of techniques. A p-value of less than 0.05 was considered significant.



留言 (0)