
記住我


At our institution, we perform approximately 160 deceased donor liver transplantations, 25 LDLTs, and 40 HPB surgeries annually. We have been performing robotic liver resections since 2016, but donor hepatectomies have been performed through open surgery, with no prior experience in laparoscopic donor hepatectomy. To ensure maximum donor safety, open donor hepatectomies have been performed by two experienced transplant surgeons working together. When initiating our robotic living donor hepatectomy program, these same two surgeons continued their collaboration. The surgeon with 20 years of HPB and transplant experience and 5 years of robotic surgery experience including hepatectomies and living donor nephrectomies was selected as the console surgeon performing the procedure, while the senior surgeon with 700 LDLT experience sat at the second console, providing guidance, particularly in determining the dissection lines for vessels and bile ducts. The bedside surgeon role was assigned to a junior surgeon who had recently completed a transplant and HPB fellowship. The team also included a surgical assistant who was well versed in robotic surgery. Over the course of one year, the entire team prepared for the robotic donor hepatectomy program. Preparation involved accumulating experience in robotic liver resections for liver tumors and cysts, including our first fully robotic right hepatectomy for a giant hemangioma. Additionally, we participated in observational visits to high-volume centers in Korea for three weeks. Our first three cases were performed as hybrid procedures, where hilar dissection, liver mobilization, and half of the parenchymal transection were conducted robotically, followed by a planned open conversion. The 4th case was successfully completed with a fully robotic approach. The 5th case underwent an unplanned open conversion due to concerns of gas embolism. The 6th to 16th cases were successfully completed with a fully robotic approach, resulting in a total of 12 fully robotic cases being completed.
Evaluation of the donor and selection criteria for the robotic approachOur selection criteria for living donors include age < 60 years old, no major comorbidities, < 20% steatosis, expected donor remnant liver volume > 30%, and expected graft-to-recipient weight ratio (GRWR) > 0.7%. We consider the right liver graft as the first choice. All living donor candidates undergo computed tomography (CT) angiogram and magnetic resonance imaging (MRI)/magnetic resonance cholangiopancreatography (MRCP) to assess vascular anatomy, volumetry, fat fraction, and biliary anatomy. For the robotic approach, we initially set stringent criteria, including age < 40 years, BMI < 25, estimated graft volume < 800 mL, and standard biliary or vascular anatomy, to ensure donor safety. After successfully completing the first four fully robotic cases, we expanded the criteria to include donors with biliary and vascular anatomic variations (Supplementary Table 1).
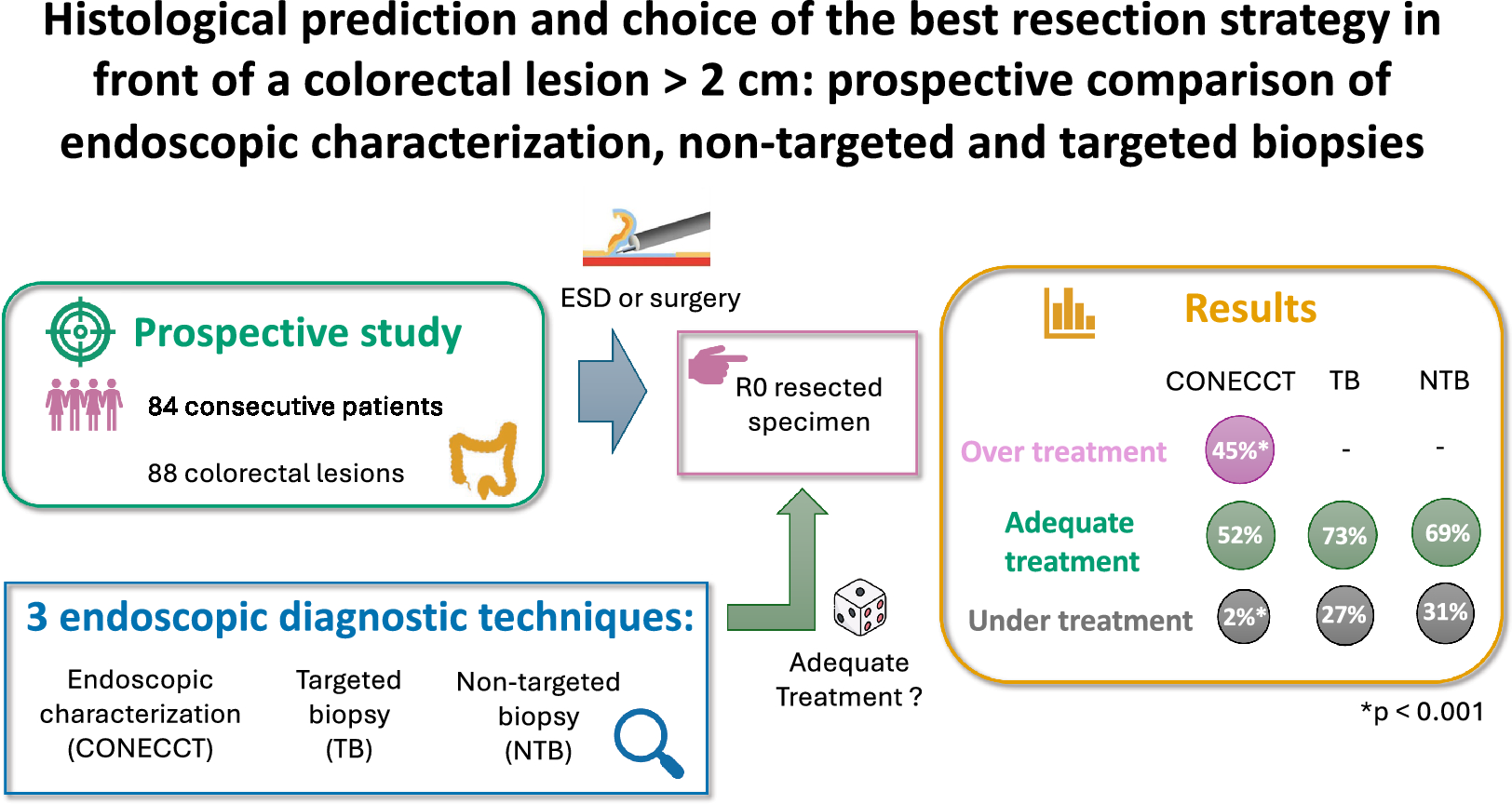
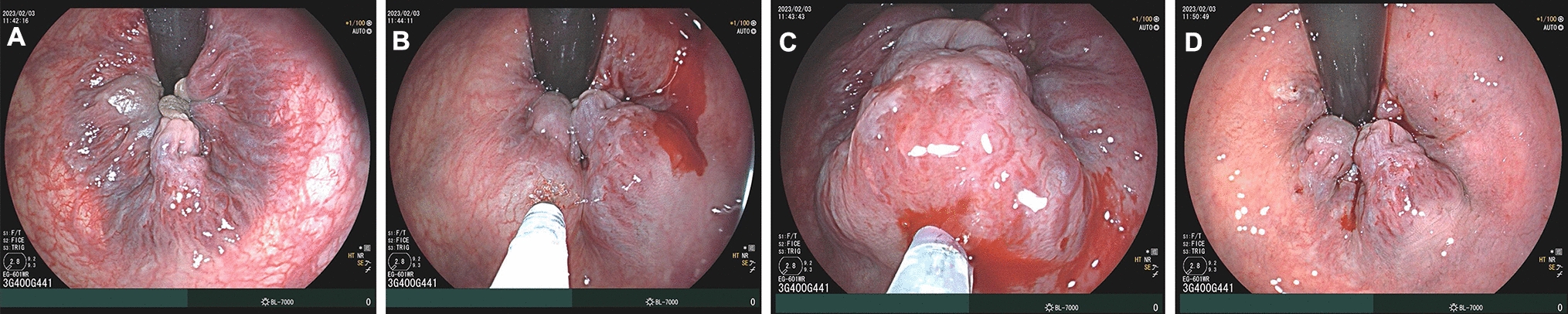
Surgical technique and intraoperative managementInformed consent was obtained from each of the donors. Our group is currently preparing a separate manuscript that will detail the surgical techniques. In summary, robotic procedures were performed using the da Vinci Xi platform (Intuitive Surgical). Port placement is shown in Fig. 1A. First, hilar dissection was performed following cholecystectomy, and the right hepatic artery and right portal vein were isolated and looped with a vessel loop (Fig. 1B). Next, parenchymal transection was performed using the Harmonic scalpel and the Micro bipolar forceps, with the help of the rubber band suspension method [11] (Fig. 1C). After most of the parenchymal transection was completed, the right hepatic duct was identified and divided with the help of indocyanine green (ICG) cholangiography (Fig. 1D, E). The right hepatic duct stump was closed with a running 5–0 PDS suture. Once the parenchymal transection and isolation of the right hepatic vein were completed, a Pfannenstiel incision was made, and a specimen bag was introduced into the abdomen. After administering heparin, the right hepatic artery was ligated using a tie and clip, and the right portal vein, right hepatic vein, and inferior vena cava ligament were divided with a vascular stapler (Fig. 1F). The graft was retrieved through the Pfannenstiel incision.
Fig. 1
Surgical technique for robotic living donor right hepatectomy. A Port placement. B Identification of the right hepatic artery and portal vein. C Parenchymal transection using rubber band suspension method. D and E Bile duct division using ICG cholangiography. F Stapling of the right hepatic vein. RHA right hepatic artery, RHD right hepatic duct, RHV right hepatic vein, RPV right portal vein
In our center, intraoperative cell salvage is routinely used during open donor hepatectomy. The decision to return salvaged blood is made by anesthesiologists based on the amount of blood loss and the donor's hemodynamics. For robotic approach, considering the typically low blood loss, cell salvage is not routinely prepared.
Study designThis cohort study was a retrospective analysis of all patients who underwent living donor hepatectomy at Virginia Commonwealth University Hume-Lee Transplant Center (Virginia, U.S.A.) between June 2022 and February 2024. This study was conducted in full compliance with the Declaration of Helsinki and was approved by the Institutional Review Board of Virginia Commonwealth University. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational studies [12].
Between June 2022 and February 2024, a total of 41 living donor hepatectomies were performed at our center. One case of left hepatectomy was excluded. Of the remaining 40 right liver donors, 3 cases that underwent planned open conversion were excluded. Ultimately, 37 cases (13 in the robotic group [12 fully robotic and 1 unplanned open conversion] and 24 in the open group) were enrolled in this study, and the patient demographics, intraoperative data, and outcomes of these two groups were compared and analyzed. Following the intention-to-treat principle, we included one case of unplanned open conversion due to gas embolism in the robotic group, as this case was initially intended to undergo fully robotic approach. Data were collected from the patient’s medical and operative records.
Demographic data included age, sex, Body Mass Index (BMI), underlying liver disease, Model for End-Stage Liver Disease (MELD)-Na score of the recipients, and imaging study results. Operative data included operation time, estimated blood loss (EBL), detailed anatomy of the graft, cold ischemia time (CIT), warm ischemia time (WIT), and biliary reconstruction technique of the recipient. The first WIT was defined as the time from cross-clamping to the backtable perfusion of the graft. The second WIT was defined as the time from the removal of the liver graft from ice to reperfusion. The anatomy of the liver graft was classified using the Huang classification [13] for the bile duct and Nakamura’s classification [14] for the portal vein. Postoperative outcomes focused on donor/recipient laboratory data, complications, and hospital stay. Postoperative complications were classified using the Clavien–Dindo (CD) classification [15]. In addition, the Comprehensive Complication Index (CCI) [16] of each donor was calculated at the time of discharge and on postoperative day (POD) 30. Bile leak was evaluated according to the International Study Group for Liver Surgery (ISGLS) definitions [17]. Early allograft dysfunction (EAD) was defined according to the criteria proposed by Olthoff et al. [18] During the study period, our center underwent several changes to the perioperative analgesia protocol (including peripheral nerve block, epidural anesthesia, and intravenous patient-controlled analgesia only). Therefore, this study was unable to evaluate pain outcomes.
Statistical analysisData are presented as the median (range) or number (percentage). The data between the two groups were compared using the Chi-square test or Fisher exact test for categorical variables and the Mann–Whitney U test for continuous variables. P values of < 0.05 was considered statistically significant. All statistical analyses were performed with R (version 3.6.1; The R Foundation for Statistical Computing, Vienna, Austria).
留言 (0)