Study design
This single-center, prospective, randomized, controlled clinical study aimed to evaluate the effect of intravenous lidocaine on SRAEs associated with ERCP in elderly patients with frailty. This study was approved by the Institutional Ethics Committee of Shanghai Shuguang Hospital (ethics approval number: 2020-says-004) and registered at Chictr. Org. cn (ChiCTR2300067796). All patients received information regarding their participation in the study and provided written informed consent.
Inclusion criteria and frailty assessment
Inpatients who scheduled for ERCP were evaluated by physicians who did not participate in endoscopic anesthesia. Patients aged > 65 and assessed for frailty as proposed by Fried et al. were included in the study [21].
The Chinese version of the Frailty Assessment Components Standardized Protocol was used. These criteria include five components: (1) Unintentional weight loss of ≥ 4.5 kg or ≥ 5% of body mass in the last year (obtained from patient, caregiver, or medical records); unexplained weight loss in the past year; (2): Weakness (assessment based on the handgrip strength measurement; interpretation of results takes into account sex and body mass index [BMI]). An electron digital dynamometer was used for grip strength measurement; (3) Exhaustion (audited information based on two questions from Center for Epidemiological Studies Depression (CES-D) scale; a score from 1 [fatigue or exhaustion felt rarely or not at all] to 4 [fatigue or exhaustion felt most of the time], 3 or 4 points means that the test is positive for decreased physical activity); (4): Slow gait (walking time over a distance of 4.57 m; interpretation of results takes into account sex and height); (5): Low physical activity (energy expenditure weekly rate calculated based on the modified questionnaire Minnesota Leisure Time Activity Questionnaire).
Patients with a Frailty Score of three or more were considered as“frail”. A Frailty Score of one or two was considered as “prefrail” and patients with zero points counted as “non-frail” [22].
Exclusion criteria
Patients were excluded if they were identified with the following risk factors: ASA grade V, STOP-BANG score ≥ 3, Mallampati airway grade 4, body mass index (BMI) ≥ 35 kg.m2, hypoxemia (pulse oxygen saturation < 90%), hypertension (systolic blood pressure > 170 mmHg, diastolic blood pressure > 100 mmHg) and hypotension (systolic blood pressure < 90 mmHg), bradycardia (heart rate < 50 beats/min), severe kidney or liver dysfunction, severe kidney or liver dysfunction, allergy to lidocaine, atrioventricular block, epilepsy and inability to give informed consent.
Sample size estimation
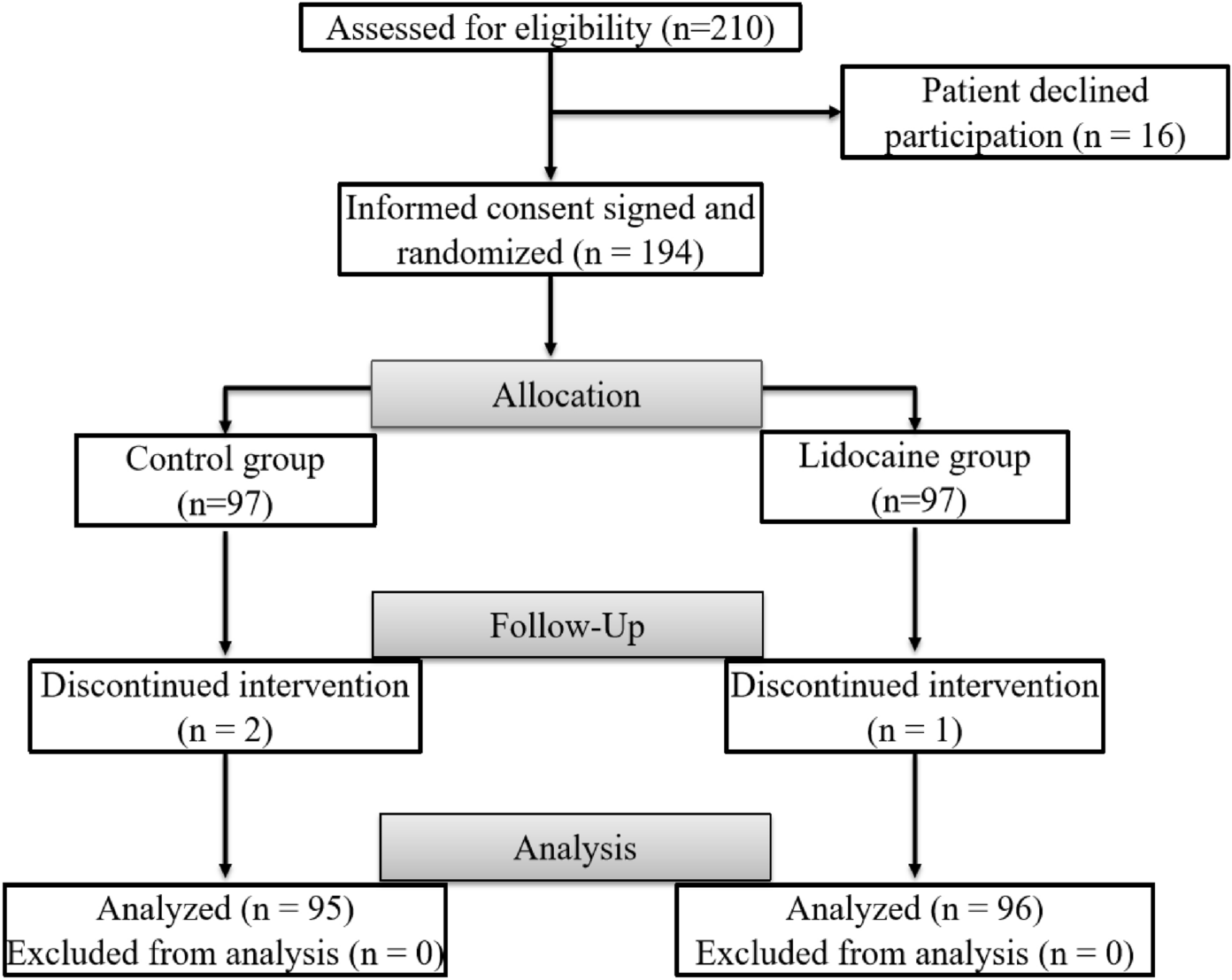
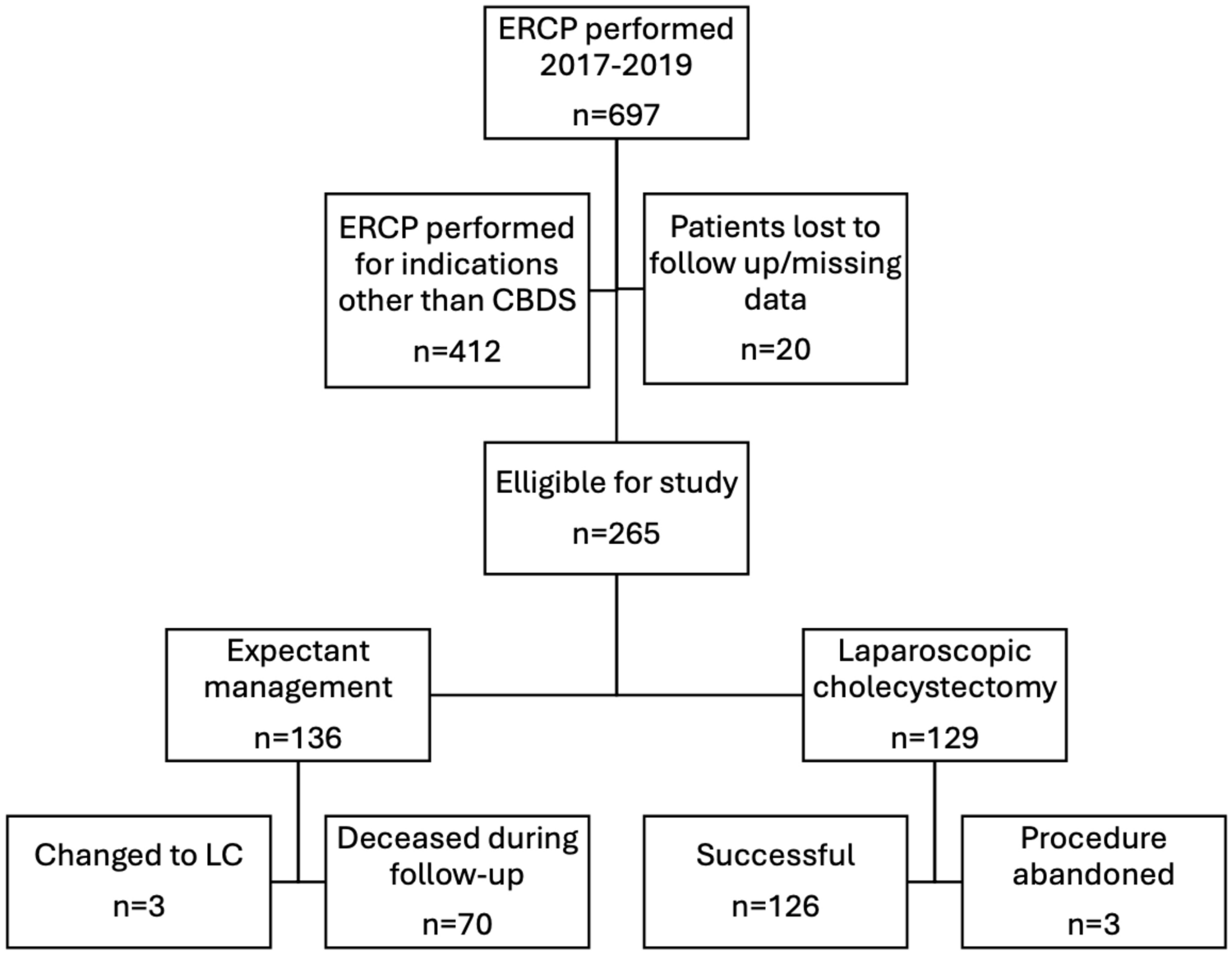
Previous prospective studies have shown that SRAEs occur in 35% of average-risk patients with MAC who undergo ERCP. To detect a reduction from this rate to 17% in the lidocaine group with a 2-tailed α of 0.05 and β 0.20 using the χ2 test, the total number needed was calculated as 186. Assuming a loss-to-follow-up rate of approximately 10%, 210 patients were enrolled.
Randomization and blinding
Using an online research randomizer (https://www.randomizer.org), patients were randomly divided into control and lidocaine groups with an allocation ratio 1:1. The randomized sequence was maintained in an opaque envelope. The drugs used in this study were prepared by a nurse and administered by another anesthesiologist. Syringes containing lidocaine or saline are identical, while others cannot identify the drug based on the solution’s appearance, color, or smell. The anesthesiologists, ERCP physicians, and patients were blinded to the grouping.
Monitoring of patients and anesthetic procedure
All ERCP procedures were performed in an endoscopy room with advanced cardiac life support. The patient was placed in the semi-prone position and provided 5 L/min of oxygen through a nasal catheter. Noninvasive blood pressure was automatically measured at 5-min intervals. SpO2, HR, respiratory rate, and ECG were continuously monitored.
The same endoscopist performed all ERCP procedures. Both groups received indomethacin (50 mg) anal plug half an hour before surgery. Sufentanil (0.1 μg/kg) and midazolam (0.01 mg/kg) were injected intravenously in the two groups before anesthesia induction. The Lidocaine group was injected intravenously lidocaine (1.0 mg/kg) followed by continuous intravenous infusion (2.0 mg/kg), while the control group received an equal volume of salt solution.
A computer-controlled infusion programmed (Graseby 3500 syringe pump, SIMS Graseby Ltd, Herts, UK) for effect site target of propofol was used to rapidly attain and maintain the sequential increase of the compartment concentration. The initial target-controlled concentration was 2.0 μg /mL, and the incremental concentration was 0.5 μg/mL. After the targeted depth of sedation reached a modified observer’s assessment of alertness/sedation scale of 1 or 2 in all patients, the endoscopist began the procedure.
During the procedure, the anesthesiologist recorded data on the patient’s basic vital signs and adverse events related to sedation during ERCP. Suppose the patient shows discomfort (involuntary somokinetic reaction, painful face) or hemodynamic changes (increase in systolic blood pressure (SBP) > 20 mmHg, increase in heart rate (HR) > 20 beats/min). In that case, the target control concentration of propofol is upregulated by 0.5 μg/mL. If the patient had hemodynamic changes (SBP < 90 mmHg or Mean arterial pressure (MAP) < 60 mmHg, HR < 50/min), the target control concentration of propofol was reduced by 0.5 ug/mL, and the cardiovascular active drug ephedrine (5 mg) was given. The endoscopist chooses whether to interrupt the operation based on their judgment.
If the patient appears hypoxemia (defined as Spo2 ≤ 90%) during the procedure, Airway support maneuvers such as chin lift or jaw thrust, nasal airway insertion, and nasal mask ventilation may be required. Severe hypoxemia (defined as Spo2 ≤ 75% or Spo2 ≤ 90%, lasting 60 s or more) or difficult-to-correct airway obstruction and laryngeal spasm are decided by the anesthesiologist whether to interrupt, switch to tracheal intubation general anesthesia or terminate the procedure.
At the end of the procedure, all medications were stopped, and the dosage was recorded. The patients were transferred to the post-anesthesia care unit, and the time to recovery was recorded. When the patient fully recovered consciousness, another researcher evaluated the degree of postoperative visceral pain using a 10-point visual analog scale (VAS). The patients’ satisfaction and endoscopists’ satisfaction of the patient’s cooperation and sedition were evaluated by a 10-point scale, and the complete satisfaction was defined as ≥ 9 points. Another observer recorded drowsiness, dizziness, nausea, vomiting, and other side effects related to lidocaine 24 h after ERCP surgery.
Study endpoint
The primary endpoint was the composite incidence of SRAEs. SRAEs were defined as any of the following: hypoxia (SpO2 < 90%) with airway maneuvers or tools (chin lifts or jaw thrusts, insertion of nasal airways, and nasal mask ventilation), hypotension requiring vasopressors, cardiac arrhythmias, interruption or termination of MAC, or change to tracheal intubation under general anesthesia.
The secondary endpoints were propofol consumption, time to recovery, VAS score, endoscopists’ and patients’ satisfaction scores, ERCP success rate, perioperative complications (mainly intraoperative reflux, aspiration, bleeding, perforation, postoperative pancreatitis, fever, pulmonary infection, and aspiration pneumonia), length of stay, and lidocaine-related adverse events (mainly cardiovascular and central nervous system adverse events caused by lidocaine).
Statistical analysis
Data were analyzed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). Categorical data were presented as percentages and were compared using the χ2 test. Continuous data are presented as standard deviation or as median and interquartile range. A 2-sampled t-test was used to compare continuous parametric data, and the Mann–Whitney U test was used for nonparametric data. A 2-sided alpha was set at 0.05 for all hypothesis tests. Multivariate logistic regression analysis was done to look for predictors of adverse events associated with sedation.



留言 (0)