The rate of bilateral breast cancer in our series was 3.6%, with MBBC constituting 2.4% and SBBC 1.2%. Our incidence of bilateral breast cancer, particularly SBBC, was comparable to those reported in the Western series [7,8,9]. Regarding synchronous bilateral breast cancer, DFS duration was similar to MBBC and unilateral breast cancer, while it was the breast cancer subtype with the shortest overall survival time. In our study, patients with metachronous bilateral breast cancer (MBBC) had a statistically significantly longer survival time compared to those with unilateral breast cancer. The overall survival (OS) durations in our series ranked as follows: MBBC had the longest survival, followed by unilateral breast cancer, and then synchronous bilateral breast cancer (SBBC). Additionally, there was a statistically significant difference in survival time between SBBC and MBBC (p = 0.027). Consequently, our findings did not support previous reports suggesting that bilateral breast cancer has a similar or better survival time compared to unilateral breast cancer [2, 9].
In the histopathological, clinical, and treatment characteristics of the patients in our series, after propensity score analysis, it was found that unilateral BC had a more advanced tumor stage (p < 0.001), a higher rate of skin involvement (p = 0.044), leading to a higher rate of neoadjuvant chemotherapy (p = 0.005), and a higher rate of receiving radiotherapy (p = 0.034). In the bilateral BC group, the statistically significant differences included a higher rate of PR positivity (p = 0.011), a higher rate of axillary curettage (p < 0.001), and a greater use of tamoxifen (p = 0.039). In the comparison of the primary tumors of patients with BBC, categorized as MBBC and SBBC, we observed a more advanced N stage in metachronous BBC (p = 0.030), a higher rate of positive surgical margins in SBBC (p = 0.007), and a higher rate of progesterone receptor (PR) positivity in the secondary tumors of SBBC (p = 0.009). Despite the more advanced N stage in MBBC, the longest survival time was observed. At the same time, SBBC had the shortest survival time, which was notable for its association with positive surgical margins and higher PR positivity. It was particularly challenging to explain the lowest survival rate observed in SBBC based on patient and treatment characteristics. A study by Kwast et al. suggested that SBBC might have an undiscovered genetic mutation, which could be significant in the cancer’s different progression. They reported that SBBC’s tendency toward tertiary cancers outside the breast could indicate that it is a distinct subtype of cancer [19].
In the literature review, studies supporting the results of our series [4, 7, 8] also reported that the overall survival (OS) time in patients with SBBC is shorter. As Holm M. et al. stated in their meta-analysis, SBBC is associated with the lowest OS, and they propose that, even though these patients may have smaller and less aggressive tumors, the presence of SBBC should be considered a poor prognostic factor [7, 8]. Additionally, Jobsen JJ et al. noted that synchronous tumors are less frequently observed. While this rate may increase with modern imaging techniques, the preference of patients with unilateral BC for bilateral mastectomy as a surgical option may reduce this likelihood [8].
In our series, while the bilateral status did not affect DFS in the multivariate Cox regression analysis when bilateral cancers were collectively compared to unilateral breast cancer for OS, it had a risk-reducing effect (by 2.1 times). When the same analysis was conducted by comparing MBBC and unilateral BC, we observed that the risk of death was reduced by 2.8 times, which was close to statistical significance. However, when SBBC was compared to unilateral BC, the risk of death increased by 2.5 times, although this increase was not statistically significant. The much better survival observed in metachronous breast cancer compared to unilateral breast cancer can be attributed to the fact that these patients are already under follow-up and, with the diagnosis of the secondary tumor, they re-enter a strict follow-up process.
In our series, risk factors affecting DFS (T4 stage, N3 stage, being PR positive) and OS (N3 stage, skin involvement, being ER positive) were identified through multivariate Cox regression analysis. However, risk factors for BBC mentioned in the literature, such as a family history of breast cancer, young age at first diagnosis, and having lobular carcinoma, were not identified as risk factors in our series. Another risk factor mentioned in the literature is the increased risk of developing BBC in patients with germline mutations in the BRCA1 or BRCA2 genes [2, 7, 20]. In our series, a germline mutation in the BRCA1 or BRCA2 genes could not be statistically analyzed due to the limited number of patients tested for it. As noted by Mruthyunjayappa S. and colleagues, since the prevalence of BRCA1 and BRCA2 mutations is very low and the tendency for prophylactic bilateral mastectomy in healthy women and prophylactic contralateral mastectomy in women with UBC is increasing, most BBC patients do not carry these mutations [2, 9].
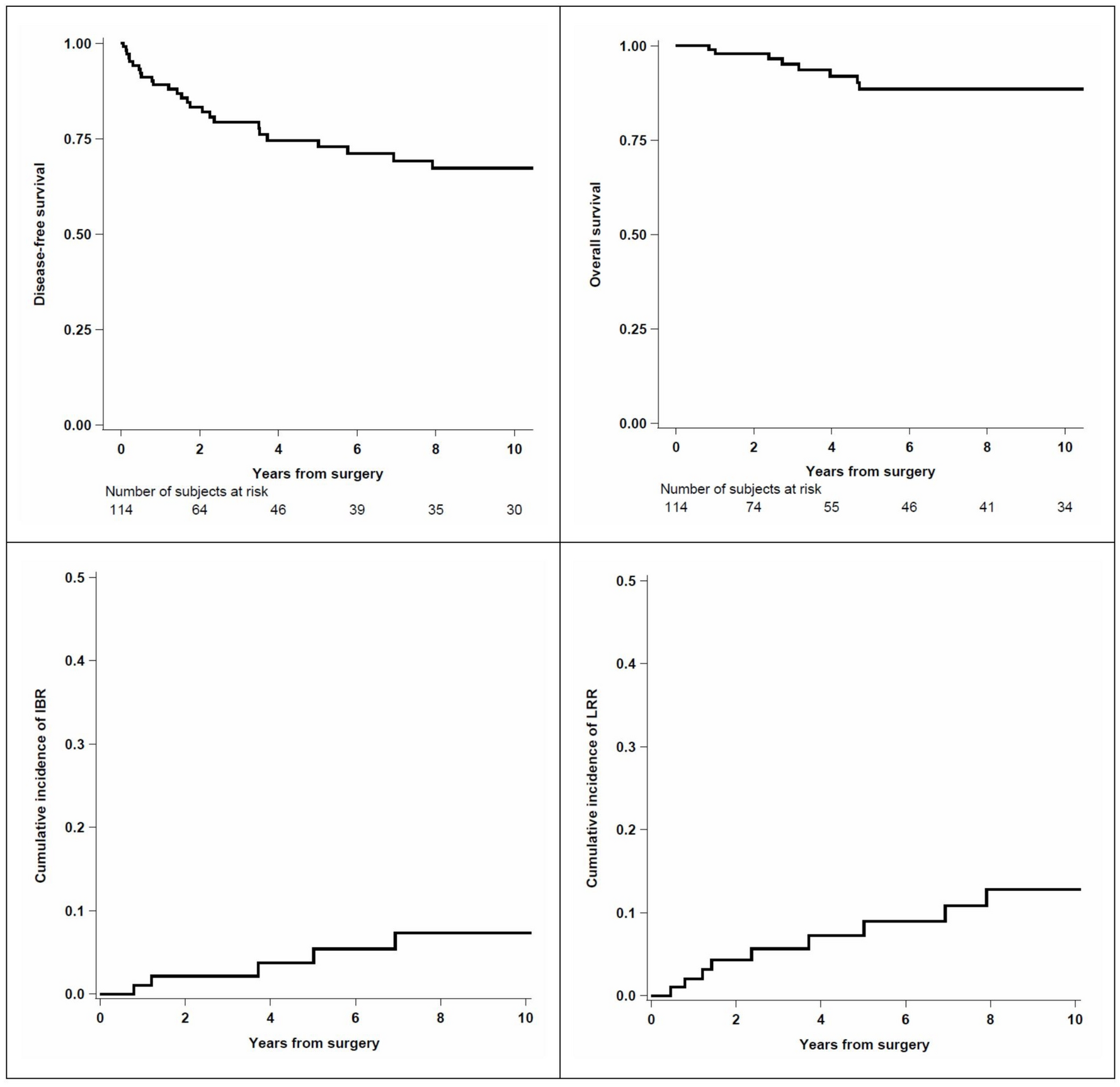
When examining Figs. 3a and 3b in our series, 75% of SBBC patients experienced recurrence/metastasis in a shorter period, and 62.5% of the patients were lost within the first 5 years. The finding that “bilaterality has no negative effect on survival.” As mentioned in studies where SBBC and MBBC are evaluated together [2, 9, 10, 19], was not surprising. Perhaps the fact that we are dealing with a subgroup with a lower incidence compared to unilateral breast cancer may have caused an imbalance in the comparisons. However, it is possible to say that propensity score analysis, a statistical method, is a golden statistical analysis method designed precisely for the evaluation of groups with numerical imbalances, such as in this case [15, 16].
There are currently no standard treatment guidelines for BBC treatment. Therefore, developing a personalized treatment plan is done by considering the patient’s age, histological subtype of the tumor, and tumor stage. Although the incidence of BBC differs between Western and Eastern countries, we see that treatment strategies, especially surgical approach options, are similar. Chen, JJ et al. [21, 22] reported that bilateral mastectomy was the primary surgical treatment option, particularly for SBBC patients, which was consistent with the findings in our series. Similarly, in the study by Beckmann et al., the number of patients who underwent mastectomy and ALND in BBC was higher, while the number of patients receiving RT was lower [23, 24]. In our study, while the surgical findings were similar, the number of patients receiving RT was higher.
In our study, the rate of axillary lymph node dissection (ALND) was 45.1% for unilateral breast cancer and 85.9% for bilateral breast cancer. More aggressive surgical approaches were preferred in the bilateral breast cancer group in terms of both local and axillary surgery. However, when comparing the T stage and N staging of unilateral breast cancer patients to bilateral breast cancer patients after propensity score analysis, the unilateral breast cancer group was found to be at a more advanced stage (Table 1). For this reason, the neoadjuvant chemotherapy option was more frequently preferred in patients with unilateral breast cancer (23.9% in unilateral breast cancer, 11.3% in bilateral breast cancer, p = 0.005).
In the series by Jia H. et al., the luminal B type was the most observed group in the bilateral breast cancer group [3]. In our series, Luminal B was also the most frequently seen subtype. Similarly, in the study by Kollias et al., which had results like ours, high-grade tumors constituted 29% of metachronous tumors, while they made up 45% and 54% of unilateral and synchronous tumors, respectively. In SBBC, tumors with a diameter ≥ 2 cm had lymph node involvement [12]. In our series, the rate of grade III was 39.4% for MBBC, 47.9% for unilateral BC, and 41.7% for SBBC. Notably, the rate of positive surgical margins in our series was higher in patients with synchronous breast cancer. This finding is significant because a considerable number of patients chose mastectomy, and both breasts were operated on simultaneously. This approach aimed to minimize surgical morbidity for both the surgeon and the patient, as well as to prevent delays in the initiation of adjuvant therapy.
Although international evidence regarding the prognostic significance of synchronous bilateral breast cancer is inconsistent, survival rates for these patients are generally found to be similar to or worse than those for unilateral breast cancer [7, 8, 23,24,25,26,27]. To better understand the reasons for the poor prognosis, researchers propose that undiscovered genetic factors may contribute, acknowledging that the low incidence rate of approximately 1% may prevent large-scale studies or randomized trials. Consequently, future research should focus on exploring these potential genetic factors [19].
Despite the small number of patients, when matched with propensity score analysis, the patient group with the lowest overall survival was the synchronous bilateral breast cancer group. Due to the wide variability in clinical and histopathological features and the time elapsed between the diagnosis of the first and second tumors [28], it has not been possible to conduct a risk analysis for synchronous bilateral breast cancer. Therefore, meticulous planning and modification of surgical and adjuvant treatment for patients with synchronous bilateral breast cancer is crucial. The discovery of genetic factors that may be identified in the coming years will also be particularly important for this patient group.
The limiting factors in our study were the retrospective nature of our series and the lack of information on BRCA-1 and BRCA-2 mutations in our patients. Although there are studies suggesting that survival outcomes for breast cancer patients with BRCA-1 or BRCA-2 mutations may be worse, similar, or better compared to non-carriers, none of the patients in our study had mutation status available for propensity score analysis, and therefore, we could not include this information in our analysis. In studies analyzing patients with BRCA1 and BRCA2 mutations, Lee et al. found that BRCA1 mutations decreased overall survival (OS) and progression-free survival (PFS), while BRCA2 mutations did not. On the other hand, Zhong et al. suggested that BRCA1 mutations were associated with worse OS, but not with PFS, and that BRCA2 mutations were not linked to either worse OS or PFS. They noted that the contradictory nature of these findings was likely due to limited statistical power [29,30,31]. However, in recent years, particularly with younger patients, we have been able to identify individuals with BRCA1 and BRCA2 mutations and have had the opportunity to provide genetic counseling, similar to the study by Liu et al. [32]. Therefore, we believe that future studies will allow us to share this information as well.



留言 (0)