
記住我
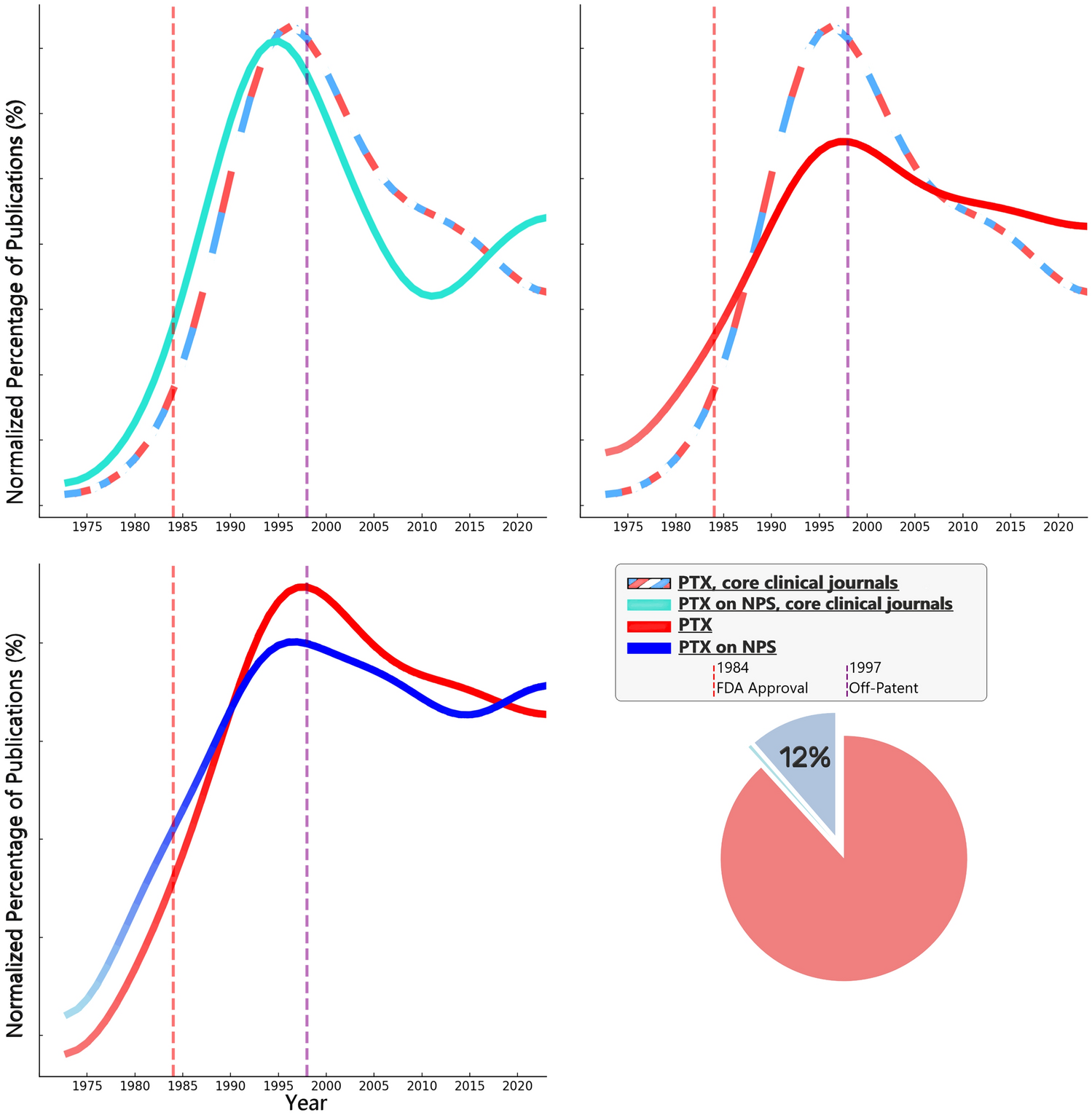
Evaluating the evolution of pentoxifylline (PTX) research publications reveals distinct patterns that correlate with key regulatory milestones, namely FDA approval in 1984 and the drug's transition to off-patent status in 1997 (U.S. 2024; U.S. 2024).
PTX publications peaked in the early and mid-1990s, with a notable decline following its transition to generic status after the loss of patent protection. This suggests that regulation-related market changes likely had a substantial influence on clinical research activity.
This trend was particularly pronounced in PubMed's core clinical journals, reflecting broader interest in PTX beyond this collection of major American clinical research journals (United States National Library of Medicine 2020; Powell and Pentoxifylline 2015; Klein-Fedyshin and Ketchum 2023).
Publications regarding PTX on psychiatric and neuropsychiatric symptoms (NPS) followed a similar trajectory, peaking before 1997 but maintaining a relatively sustained proportion of overall PTX research over the years. Despite the decline in PTX studies after 1997, research on NPS has continued to account for around 11% of all PTX publications, indicating enduring interest in this domain. In recent years, a relative increase in research regarding PTX on NPS, possibly driven by emerging evidence, contributes to the rationale for this study. These patterns are visualized in a compound Figure (Fig. 1).
Fig. 1
This compound figure consists of 4 sub-figures: three line graphs and one pie chart, each illustrating different aspects of publication patterns related to pentoxifylline (PTX) in human research on PubMed. Below is a detailed description: Top Left Graph (PTX General vs. NPS, in CCJ): Y-Axis: Normalized Percentage of Publications (%), X-Axis: Year (1973–2023).—Lines: Alternating Red-White-Blue: PTX publication trend in core clinical journals (CCJ). Turquoise line: PTX publication trend on neuropsychiatric subjects (NPS) within CCJ. Annotations: Vertical dashed red line: FDA approval of PTX (1984). Vertical dashed purple line: PTX off-patent year (1997). Top Right Graph (CCJ vs. All Journals): Axes and annotations: Same as above.—Lines: Alternating Red-White-Blue: PTX publication trend in CCJ. Solid Red: PTX publication trend across all journals. Bottom Left Graph (PTX General vs. NPS): Axes and annotations: Same as above.—Lines: Solid Red: PTX publication trend in general. Solid Blue: PTX publication trend on NPS. Pie Chart (Bottom Right): Proportion of PTX publications on NPS: Shaded bluish segment representing 12% of total publications
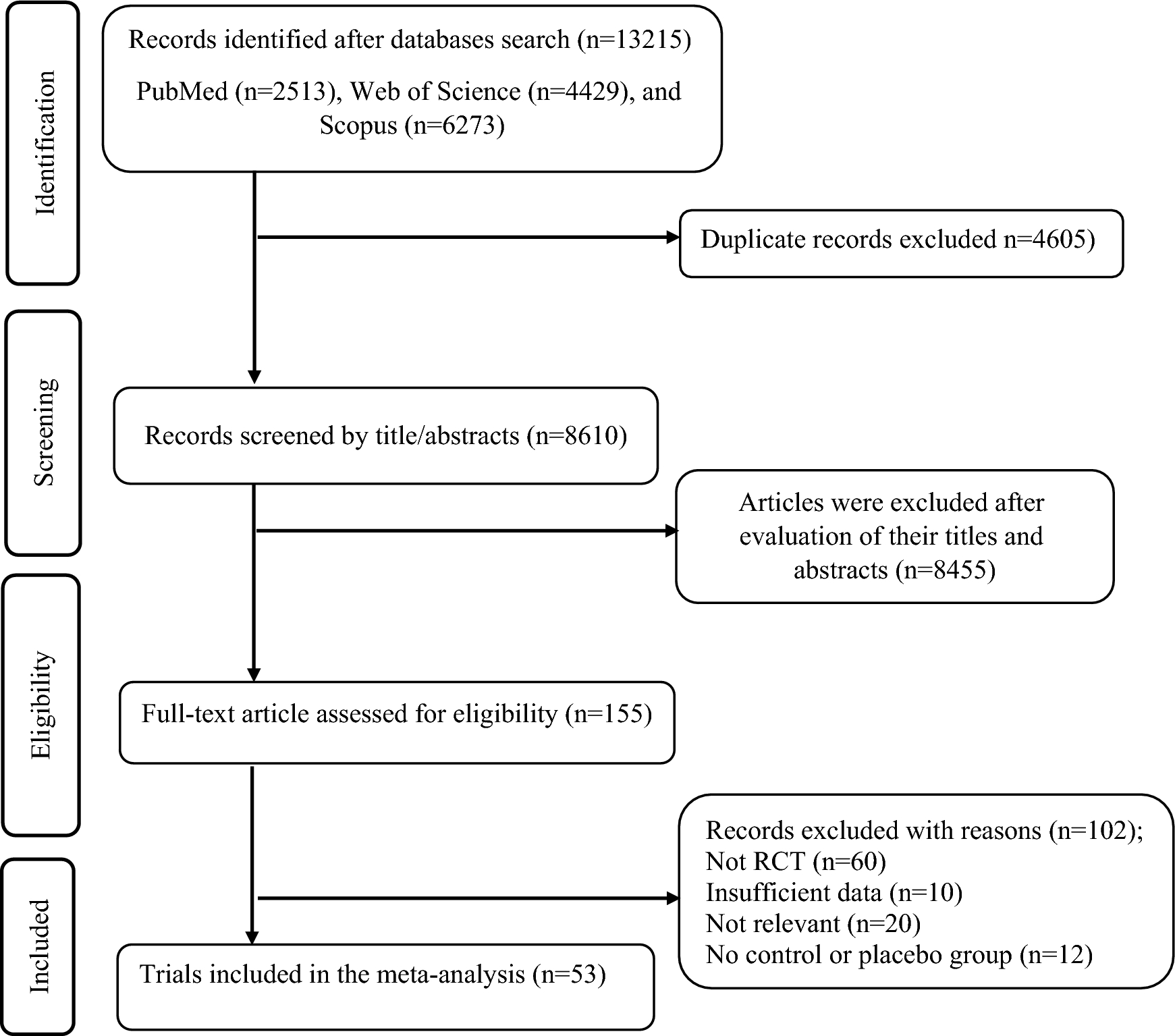
Results of the main searchOn 25 September 2024, a systematic updated search of four major electronic databases identified 5,607 studies: EMBASE (n = 711), PubMed (n = 1060), Scopus (n = 2953), and Web of Science (n = 883). After removing 331 duplicates and 4,911 records by search settings, 365 records were screened, resulting in 34 full-text articles assessed for eligibility. Ultimately, 21 randomized controlled trials (RCTs) were included in the review.
Curation is outlined in a flowchart (Fig. 2).
Fig. 2 Included studies
Included studiesThe list of the 21 included RCTs:
Merza Mohammad 2024 May (Merza Mohammad et al. 2024), August (Mohammad et al. 2024), Farajollahi 2021 (Farajollahi-Moghadam et al. 2021), (Yasrebi et al. 2021), (El-Haggar et al. 2018),
Sinichi (2023), Pavlov (2021), Al-Nimer (2019), Procházková (2018), Escolar (2012), Akhondzadeh (2010),
(1997), Bayer (EPMID) (1996), Black (1992), Blume (1992), Hartmann (1988), (Ghose 1987), Parnetti (1985), Parnetti (1984), Janaki (1980), Harwart (1979).
Theme-wise, studies will be addressed as follows: first we will introduce the studies on depression, mainly major depressive disorder (MDD), followed by the studies focusing on cognitive impairment (CI) and lastly a smaller group of neurodevelopmental and other neuropsychiatric conditions.
Risk of bias (ROB) appraisal:
Visualized Quality/ ROB assessment for 21 RCTs included in the study is provided in the following Fig. 3. It is notable that approximately half of the studies were assessed to have a moderate or high risk of bias, mainly in the older studies pertaining to cognitive impairment.
Fig. 3
Risk of bias domains and judgment for the included RCTs, using the ROB2 tool
Studies in affective disordersFive randomized, double-blind, placebo-controlled trials used PTX versus placebo for treating depression in 360 patients (Merza Mohammad et al. 2024; Mohammad et al. 2024; Farajollahi-Moghadam et al. 2021; Yasrebi et al. 2021; El-Haggar et al. 2018). Four focused on major depressive disorder (MDD), with two investigating moderate depression (El-Haggar 2018, Yasrebi 2021) and two examining severe depression (Farajollahi 2021, Merza Mohammad May 2024), while one study (Merza Mohammad August 2024) addressed bipolar I/II with treatment-resistant depression (TRD), classified as severe depression.
The Hamilton Rating Scale for Depression (HAM-D-17) was used to assess depressive symptoms, applied as an inclusion criterion in MDD, and the response rate was uniformly defined as a ≥ 50% drop in HAM-D-17 scores.
Regarding MDD, in three of the four studies, PTX was used as an adjuvant to a selective serotonin reuptake inhibitor (SSRI). However, even the one study that used PTX as a sole intervention also reported a significant reduction in depressive symptoms compared to placebo, but—unlike the other studies—it did not achieve a significant intergroup difference in response rates. None of the studies showed a significant difference between PTX and placebo in terms of side effects.
The last and latest study focused not on MDD but on bipolar I/II patients with severe, treatment-resistant depression (TRD), using PTX as a sole intervention. In this 12-week RCT, no significant overall difference in HAM-D-17 score reduction was observed between PTX and placebo. Response rates were not significantly different between groups overall, but were higher for PTX in the high-CRP subgroup and lower in the low-CRP subgroup. PTX significantly reduced CRP, TNF-α, and IL-6 within its group, while the placebo group showed no significant reductions. Intergroup, only CRP showed a significant difference. The researchers suggested that PTX may be more effective in patients with elevated inflammatory status due to its strong anti-inflammatory effects.
Characteristics and summaries of these studies are presented here in Table 1 in a concise form, and in an extended Table in the supplementary file. Figures 4, 5, and 6 present a statistical synthesis of these studies regarding HAM-D score reduction, response rate, and remission rate.
Table 1 Concise presentation of depression RCTsFig. 4
The meta-analysis evaluates the mean difference in HAMD score reductions in patients with depression treated with Pentoxifylline (PTX) alone or combined with Selective Serotonin Reuptake Inhibitors (SSRI). Two studies on PTX alone (Merza Mohammad 2024 August, Yasrebi 2021) show a pooled mean difference of − 2.89 [95% CI (− 7.00, 1.21), p = 0.17] with significant heterogeneity (I2 = 86%). Three studies on PTX + SSRI (El-Haggar 2018, Farajollahi-Moghadam 2021, Merza Mohammad 2024 May) show a pooled mean difference of − 3.41 [95% CI (− 4.09, − 2.72), p < 0.00001] with no heterogeneity (I2 = 0%). The overall pooled mean difference across all studies is − 3.44 [95% CI (− 4.63, − 2.24), p < 0.00001] with moderate heterogeneity I2 = 67%
Fig. 5
Response rate in depression with Pentoxifylline (PTX) alone or combined with Selective Serotonin Reuptake Inhibitors (SSRI). Two studies assessing PTX alone (Merza Mohammad 2024 August, Yasrebi 2021) show no significant effect with a pooled risk ratio (RR) of 1.42 [95% CI (0.56, 3.57), p = 0.46] and no heterogeneity (I2 = 0%). In contrast, three studies (El-Haggar 2018, Farajollahi-Moghadam 2021, Merza Mohammad 2024 May) evaluating PTX + SSRI show a significant increase in response rate with a pooled RR of 1.65 [95% CI (1.33, 2.05), p < 0.00001] and no heterogeneity (I2 = 0%). Overall, the pooled RR across all studies is 1.58 [95% CI (1.30, 1.93), p < 0.00001] with no significant heterogeneity (I2 = 0%)
Fig. 6
Remission rate in MDD patients was evaluated through a meta-analysis of 3 studies (236 participants total). The synthesized risk ratio (RR) was 2.04 (95% CI 1.55–2.69, p < 0.00001), showing a significantly higher remission rate in the Pentoxifylline group compared to the control, with no heterogeneity detected (I2 = 0%). The subsequent forest plot displays a sensitivity analysis that excluded the Yasrebi 2021 study, which had minimal influence on the overall analysis. This adjustment did not impact the significance of the results, as the pooled risk ratio remained at 2.04 (95% CI 1.54–2.70, p < 0.00001) with zero heterogeneity (I2 = 0%)
Studies pertaining to cognitive impairmentOlder studies conducted in older populations evaluated the efficacy of pentoxifylline (PTX) in mitigating cognitive deterioration across various neurocognitive and cerebrovascular conditions, with sample sizes ranging from approximately 40 to 290 participants. All ten of these studies were randomized controlled trials (RCTs), with the majority being placebo-controlled and most reported following double-blind methodologies, although some varied in design (Parnetti et al. 1997, 1985; Bayer 1996; Black et al. 1992; Blume et al. 1992; Hartmann and Tsuda 1988; Ghose 1987; Janaki 1980; Harwart 1979).
The usual dose of pentoxifylline, 400 mg tablets taken three times daily, was used in almost all of the studies. The outcomes evaluated included cognitive function assessments, mental state evaluations, and clinical symptoms relevant to cerebrovascular insufficiency and dementia. Scales such as the Mini-Mental State Examination (MMSE) and the Sandoz Clinical Assessment-Geriatric (SCAG) were commonly used to quantify these outcomes.
Significant improvements in cognitive and clinical parameters were reported in most studies, with PTX consistently showing a beneficial effect compared to placebo or other comparators. Generally, no significant differences in side effects were reported between the PTX and placebo groups, indicating a favorable safety profile for PTX.
Detailed characteristics and outcomes of these studies are presented in Table 2, with extended data available in the supplementary file. Quantifiable results pertaining to cognitive impairment are meta-analyzed in Fig. 7.
Table 2 Characteristics of studies on cognitive impairmentFig. 7
This meta-analysis evaluates the mitigation of cognitive deterioration across 7 studies (totaling 506 participants). The pooled standardized mean difference (SMD) was − 1.03 (95% CI − 1.61 to − 0.44, p = 0.0006), indicating a significant reduction in cognitive decline in the experimental group (Pentoxifylline) compared to the control (placebo). The analysis revealed high heterogeneity (I2 = 86%). The second part of the figure presents a sensitivity analysis that excluded the study by Black 1992, which was identified as a major source of heterogeneity. After this exclusion, the results remained significant, with a pooled SMD of − 0.66 (95% CI − 0.98 to − 0.34, p < 0.0001), and heterogeneity was substantially reduced (I2 = 47%)
Studies on neurodevelopmental and other neuropsychiatric conditionsStudies of PTX in the domain of neuropsychiatry are not limited to depression and cognitive impairment but extend to neurodevelopmental disorders such as autism and schizophrenia, as well as other neuropsychiatric conditions like asthenia, anxiety, and NPS-related quality of life (QOL) (Sinichi et al. 2023; Pavlov et al. 2021; Al-Nimer et al. 2019; Procházková et al. 2018; Escolar et al. 2012; Akhondzadeh et al. 2010).
In almost all of these studies, PTX induced notable improvements. The characteristics of the studies are summarized in Table 3.
Table 3 Brief description of studies on neurodevelopmental and other neuropsychiatric conditionsMeta-analysesFurther meta-analysis is in the supplementary.
留言 (0)