Data collection and patient characteristics
We extracted the Affymetrix microarray and clinical details of patients with DLBCL and healthy individuals from the GEO database (https://www.ncbi.nlm.nih.gov/geo). Healthy control data were obtained from the GTEx database (https://gtexportal.org/home/). Dataset GSE10846 comprised 420 DLBCL patient microarrays using the GPL570 platform. We collected patient characteristics and survival data and discarded incomplete datasets. The transcriptional values in fragments per kilobase of exon per million reads mapped of GSE10846 dataset were log 2 transformed into transcript per kilobase of exon model per million mapped reads via the “scale” method provided in the “limma” R 4.2.1. If a gene was repeated in the database, we reserved a row for that gene by calculating the mean value. Clinical data were obtained from GSE10846, and 114 patients with incomplete clinical information were excluded. We used the online GEPIA platform (http://gepia.cancer-pku.cn/index.html) to differentiate CDK1 mRNA expression between patients with DLBCL and healthy subjects. Raw datasets were normalized and log2 transformed via the “limma” R package (v4.2.1). The average value was retained for repeated genes in the dataset.
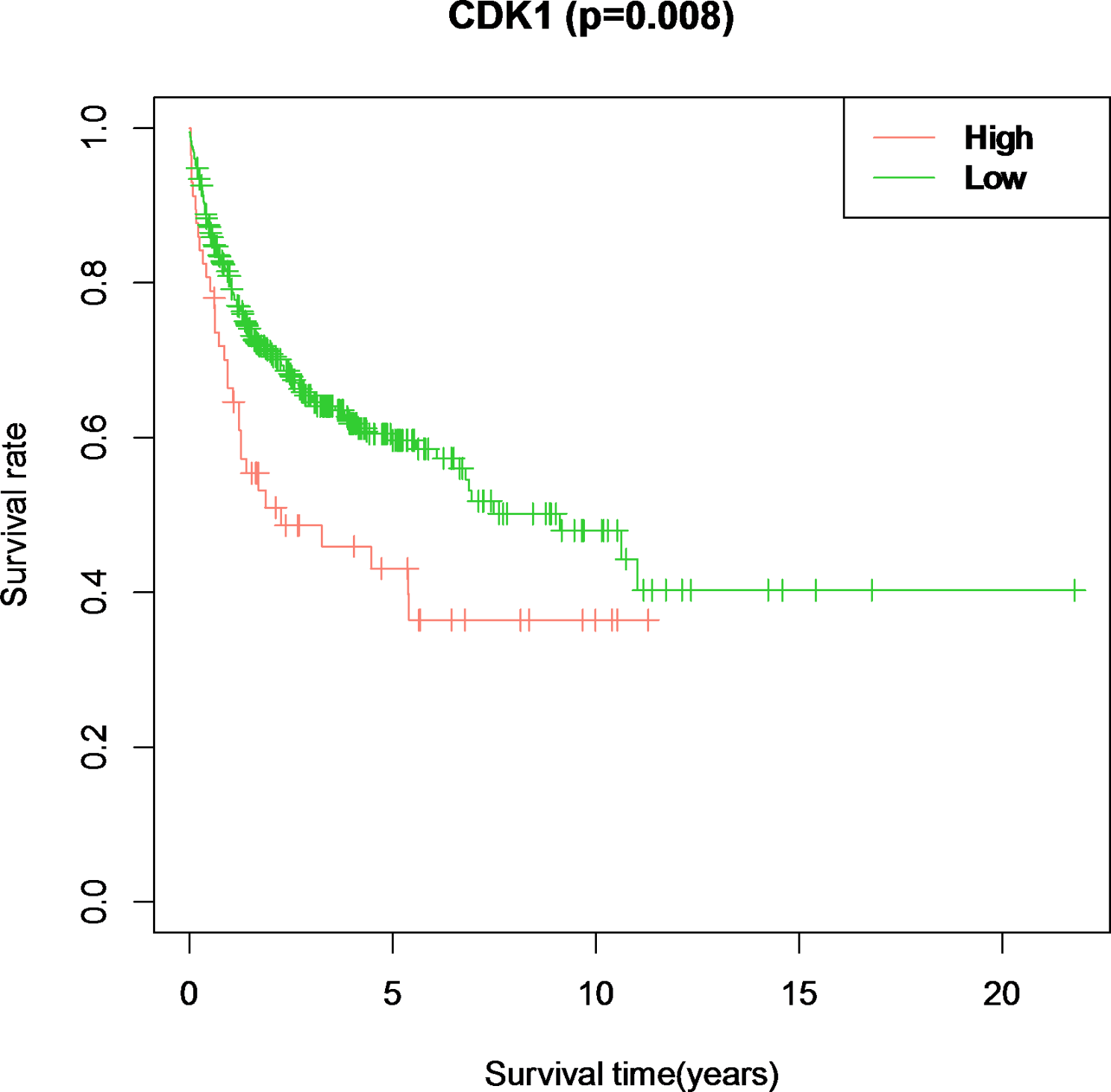
Prognostic value of CDK1 in DLBCL patients
Using the X-tile bioinformatics tool, we established a 7.6 CDK1 threshold for prognosis prediction (Supplementary Materials ). Subjects were categorized into CDK1low (≤ 7.6; N = 45) or CDK1high (> 7.6; N = 261). A comparative analysis of the clinical attributes of the cohort was conducted. We employed two-sided log-rank tests and Kaplan-Meier survival analysis to discern overall survival(OS) disparities between cohorts. Statistical significance was set at P < 0.05. Furthermore, Cox regression models (both Univariate and multivariate) were used to determine the prognostic significance of CDK1 expression and other clinical factors.
IHC analysis
We obtained lymphoma tissue samples from patients with DLBCL and healthy lymph node tissues at the Affiliated Huaian No.1 People’s Hospital of Nanjing Medical University. Tissue preparation included formalin fixation, paraffin embedding, and slicing into 3-µm sections. Following specific preparation procedures, tissues were treated with an anti-CDK1 antibody (1:500 dilution; Abcam, ab133327), and the results were interpreted by two independent pathologists. The imaging magnification was set at 20×. The staining section were reviewed and scored as follows by two pathologists: Cells with < 1% staining was scored as negative staining (-,0); cells with 1–33% staining was scored as (+,1); cells with 34–67% staining was scored as (++,2); cells with 67–100% staining was scored as (+++,3).
Cell culture and reagents
The DLBCL cell lines U2932, SU-DHL-6, and Su-DHL-4 were sourced from Shanghai Zhong Qiao Xin Zhou Biotechnology Co., Ltd. and cultivated under specified conditions (cultured in RPMI-1640 medium [Gibco, CA, USA] containing 10% fetal bovine serum at 37 °C in a 5% CO2 incubator). The CDK1 inhibitor, Ro-3306, was obtained from MedChemExpress Co., Ltd.
CCK-8 assay
The proliferation of DLBCL cell lines was assessed using the CCK-8 assay (PROTEINBIO, Nanjing, China). The U2932, Su-DHL-6, and Su-DHL-4 cell lines were cultured in 96-well plates at a seeding density of 1 × 104 cells per well. The cells were exposed to varying concentrations of Ro-3306 or 0.1% DMSO for 24 h. Next, a volume of 10 µl of CCK-8 solution was introduced into each well, followed by an incubation period of 4 h. Absorbed light was detected at a wavelength of 450 nm was ultimately accomplished using a microplate reader capable of measuring the entire wavelength range.
Cell apoptosis analysis
The YF-488 Annexin V-FITC and PI Apoptosis Detection Kits (P6002) were procured from PROTEINBIO Biotech Co., Ltd. (Nanjing, China). DLBCL cells were cultured in 6-well plates at a density of 1 × 106 cells/well. Cells were exposed to varying concentrations of 10 µM Ro-3306 or 0.1% DMSO for 24 h. Subsequently, the cells underwent three rounds of washing with cold PBS, followed by centrifugation at 1000 rpm for 5 min. In each tube, 5 µl of YF-488-Annexin V and 5 µl of PI staining solution were added. The tubes were incubated in the dark at room temperature for 15 min. Next, 400 µL of binding buffer was introduced, and the cells were subjected to flow cytometry analysis using the BD FACSCanto II instrument located in CA, USA.
Statistical analysis
Data analysis was performed using R software (version 4.2.1) and SPSS 26.0. Group-based categorical variable differences were assessed using the Mann–‒Whitney U test or chi-squared test. Kaplan-Meier analysis was performed to determine the relationship between CDK1 expression and OS. Survival outcomes between the CDK1low and CDK1high groups were compared using Kaplan–‒Meier survival curves and the log-rank test. To ascertain the optimal CDK1 cutoff, X-tile software (version 3.6.1; Yale University, New Haven, CT, USA) was used to determine. Both univariate and multivariate Cox proportional hazards models were used to identify the critical prognostic indicators. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated. Significant factors from the univariate survival analyses, recognized by a p-value of less than 0.05, were then considered for multivariate analysis to confirm CDK1’s prognostic significance. Statistical significance was defined as a two-tailed P-value < 0.05.


留言 (0)