
記住我



We identified 1,986 AEs related to lecanemab, affecting 868 patients, with an average of 2.3 AEs per patient. Of these patients, 203 experienced serious AEs, including 22 deaths. Patients were distributed from 2023 through the second quarter of 2024. Age information was available for 697 patients (mean age 73.4 ± 7.7 years), and 478 patients were specified to be females (Table 1).
Table 1 Characteristics of the patients submitted to the US FDA Adverse Event Reporting System for lecanemabFor 90 different AEs, at least four reports were recorded. The most frequently reported AEs were headache (n = 193, 12.00%) with mean time-to-onset of 5.2 days, chills (n = 100, 6.22%) with mean time-to-onset of 1.03 days, fatigue (n = 93, 5.78%) with mean time-to-onset of 9.84 days, ARIA-E (n = 91, 5.66%) with mean time-to-onset of 206.85 days, ARIA-H (n = 70, 4.35%) with mean time-to-onset of 127.07 days, infusion-related reaction (n = 66, 4.10%) with mean time-to-onset of 15.26 days, pyrexia (n = 65, 4.04%) with mean time-to-onset of 0.87 days, confusional state (n = 64, 3.98%) with mean time-to-onset of 48.05 days, nausea(n = 63, 3.92%) with mean time-to-onset of 3.97 days, dizziness (n = 51, 3.17%) with mean time-to-onset of 10.4 days (online supplementary Table 1). The characterisation of deaths is provided in Table 2. The time-to-onset distribution is shown in the online supplementary Fig. 1.
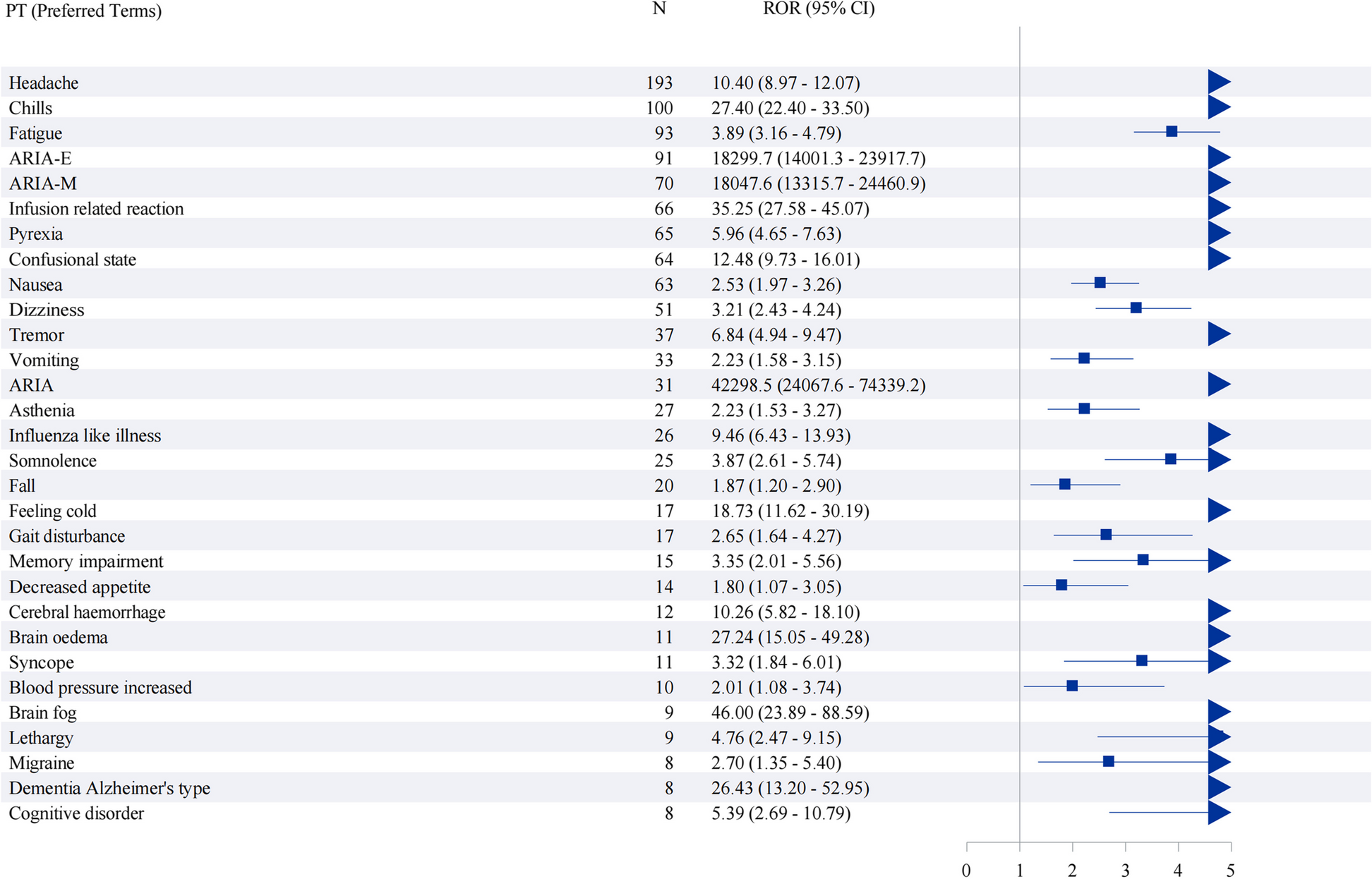
Table 2 Characterisation of deaths for US Adverse Event Reports submitted to the US FDA Adverse Event Reporting System for lecanemabDisproportionality analysesTable 3 presents disproportionality estimates for lecanemab-related AEs grouped according to the four predefined categories. AEs expected with detected signals are those mentioned in the lecanemab label or revealed in clinical trials, such as ARIA-E, ARIA-H, nausea, and chills. AEs categorised as disease-expected are highly likely to be associated with the disease itself, such as brain fog, lethargy and disorientation. Unexpected AEs include tremor, migraine, and pancreatic carcinoma. Figure 1 is a forest map showing the top 30 reported AEs, which were statistically significant. Safety signals were detected for a large number of AEs, such as ARIA (ROR 42298.55, 95% CI 24067.60, 74,339.24; IC 14, 95% CI 4.35,5.65), ARIA-H (ROR 18047.56, 95% CI 14001.27, 23,917.73; IC 13.37, 95% CI 5.73, 6.55), ARIA-E (ROR 18299.69, 95% CI 14001.27, 23,917.73; IC 13.37, 95% CI 6.15, 6.87), infusion-related reaction (ROR 35.25, 95% CI 27.58, 45.07; IC 5.09, 95% CI 4.15, 4.87), chills (ROR 27.4, 95% CI 22.40, 33.50; IC 4.7, 95% CI 4.09, 4.68).
Table 3 Safety signals for lecanemab-related adverse events with more than four counts are classified into four groupsFig. 1
The Forest Map Showing the Top 30 Safety Signals. We used disproportionality approaches: the reporting odds ratio (ROR). The ROR was considered statistically significant if the lower limit of the confidence intervals (CIs) was greater than 1. We shows the top 30 reported adverse events which were statistically significant
Sex Differences in lecanemab AEsThe most common safety signals were similar in males and females. However, ARIA was more likely to be reported in female patients, whereas chills, blood pressure increased, Corona Virus Disease 2019 (COVID-19), asthenia and pyrexia were more likely to be reported in male patients (p < 0.05) (online supplementary Fig. 2; online supplementary Table 2a, b).
Serious versus Non-Serious AEsThe time-to-onset has a significant difference between serious and non-serious AEs (p < 0.0001) (Fig. 2). Likewise, the patients with serious AEs were more likely to receive polypharmacy for Alzheimer’s disease (p = 0.009), aspirin (p < 0.001), acid-suppressing medications (p = 0.030), statins (p < 0.001), antidepressant (p = 0.015) or benzodiazepines (p = 0.038) compared to patients with non-serious AEs. By contrast, age and sex did not differ between groups (p = 0.076 and p = 0.448, respectively). ARIA-E, ARIA-H, cerebral haemorrhage, pneumonia, fall, syncope, hyperhidrosis, loss of consciousness and dehydration were more likely to be reported as severe. In contrast, headache, fatigue, chills, pain, somnolence and dizziness were more likely to be reported as non-serious (online supplementary Fig. 3).
Fig. 2
The Time-to-onset Difference Between Serious and Non-serious AEs. Legends: The time-to-onset difference between serious and non-serious AEs was analysed using the Wilcoxon Test. The result shows that time-to-onset significantly differs between serious and non-serious AEs(p < 0.0001)
Sensitivity analysesAfter analysing donepezil as a comparator for disease-related AEs, safety signals were not detected for fatigue, poor quality sleep, and asthenia. However, signals were identified for other disease-related AEs compared to the list of AEs seen for lecanemab, except for brain fog and increased lacrimation, which were not reported. When using aducanumab as a comparator, safety signals were found for confusional state, disorientation, memory impairment, falls, and lethargy. At the same time, fatigue and somnolence, along with other unreported AEs, showed no signals. We identified several safety signals for lecanemab, donepezil, and lecanemab, including confusional state, memory impairment, lethargy, dementia Alzheimer's type, disorientation, cognitive disorder, anger, aphasia, abnormal dreams, somnolence, fall, decreased appetite, heart rate decreased, pallor and incontinence (online supplementary. Table 3).
留言 (0)