Study design and population
This study was conducted at Chang Gung Memorial Hospital, Chiayi, Taiwan, from January 2018 to January 2023. Serum specimens and clinical data were prospectively collected and retrospectively examined for serum cytokines, and their correlations with clinical information were analyzed. We enrolled patients diagnosed with primary or recurrent EOC who were scheduled to undergo CRS/HIPEC for indications including: [1] neoadjuvant chemotherapy followed by interval debulking surgery and HIPEC, and [2] recurrent ovarian cancer with planned secondary CRS and HIPEC.
The exclusion criteria were: [1] age below 20 or above 75 years; [2] preoperative Eastern Cooperative Oncology Group (ECOG) performance status > 2; [3] patients undergoing palliative HIPEC for ascites control without curative intent; and [4] patients in whom optimal debulking surgery could not be achieved.
This study received approval from the Institutional Review Board of Chang Gung Memorial Hospital (approval code 202001607A3), and it met the guidelines set by the Helsinki Declaration. Written informed consent was obtained from all enrolled patients.
CRS/HIPEC procedure
All participants underwent a standardized CRS/HIPEC procedure performed by a multidisciplinary team (MDT) [12]. CRS was performed via a midline laparotomy. Post CRS, HIPEC was administered using the closed method with a Performer™ HT intraperitoneal hyperthermia system (RanD Biotech, Medolla, Italy). The perfusate comprised a mixture of normal saline and pentastarch (Haes-steril, 60 mg/mL, Meda, Sweden) at a concentration of 10% (3:1). The perfusate was administered at a dose of 2 L/m2 of body surface to achieve effective distribution within the peritoneal cavity. Chemotherapy infusion began once an intra-abdominal temperature of 41–43 °C had been reached, and HIPEC lasted for 60 min. After completion of HIPEC, the intra-abdominal chemotherapy drugs were drained.
The HIPEC regimen was chosen based on the patient’s clinical status. For individuals with primary or platinum-sensitive recurrence, a HIPEC regimen based on cisplatin was used. For those with platinum-resistant recurrence, a HIPEC regimen not based on cisplatin was used.
Study protocol and circulating cytokine measurements
The patients were recruited into the study within 1 month before their scheduled surgery after undergoing a comprehensive review by the MDT. Preoperative recruitment ensured timely enrollment, and pretreatment blood samples were routinely collected either during the preoperative evaluation or at the induction of anesthesia. A second blood sample was obtained on postoperative day 7. After collection, the samples were centrifuged at 2,600 x g for 8 min at 22 °C, and then immediately frozen and stored at -80 °C until further analysis.
CA-125 was routinely determined in all patients. In addition, with informed consent, extra serum was obtained for future research purposes. Customized MILLIPLEX MAP Human Cytokines/Chemokines/Growth Factor Magnetic Bead Panels (Millipore Corp., Billerica, MA) were used to assess a panel of candidate cytokine and chemokine concentrations. Cytokines that exhibited very low or undetectable concentrations in the patients were excluded from subsequent analysis. This selection process ensured a focus on cytokines with concentrations that were relevant when analyzing their association with the studied outcomes. The change in cytokine expression (cytokine_Change) represented the difference between post-CRS/HIPEC and baseline data, calculated as the post-CRS/HIPEC value minus the baseline value.
Clinical data collection
The case manager meticulously documented comprehensive patient-related information, operative details, postoperative outcomes, and pathology, all of which were thoroughly evaluated by the MDT committee. The patient data collected included demographics, pre-existing comorbidities such as diabetes, hypertension, and hepatitis, ECOG performance status, cancer type and disease status (primary or recurrence, histological type and grade, and peritoneal carcinomatosis index (PCI) [13]), and CRS/HIPEC parameters (chemotherapy regimen, perfusate, cytoreduction time, duration, blood loss, intraoperative blood transfusion, completeness cytoreduction (CC) score [13], and perioperative temperature).
Immunohistochemical (IHC) staining and tissue microarray (TMA)
Tissue specimens were obtained from individuals enrolled under the IRB-approved protocol (202202169A3C601) and provided by the Research Specimen Processing Laboratory, Chang Gung Memorial Hospital, Chiayi. TMAs were prepared from these specimens by the hospital’s histology lab, with each TMA containing two independent 1.5 mm cores per tumor.
IHC was performed on the TMAs using the Leica Bond MAX automated immunostainer to evaluate GROα, CXCR2, MCP-1, and CCR2α expression. Sections were first treated with 3% hydrogen peroxide to block endogenous peroxidase activity. They were then incubated with the following primary antibodies: anti-GROα (Abcam ab86436, 1:200 dilution); anti-CXCR2 (Proteintech Cat no: 20634-1-AP, 1:200 dilution); anti-MCP-1 (Abcam ab9669, 1:200 dilution); and anti-CCR2α (Proteintech Cat no: 16153-1-AP, 1:400 dilution). Subsequently, sections were labeled with horseradish peroxidase-conjugated secondary antibodies. Protein visualization was achieved using 3,3′-diaminobenzidine as a chromogen.
TMA slides were scanned using the Hamamatsu NanoZoomer S360 MD Digital Slide Scanner System at 40x magnification, with a resolution of 0.23 μm per pixel. The expression levels of the studied markers were evaluated based on staining intensity (scoring with 0, 1, 2, and 3).
Statistical analysis
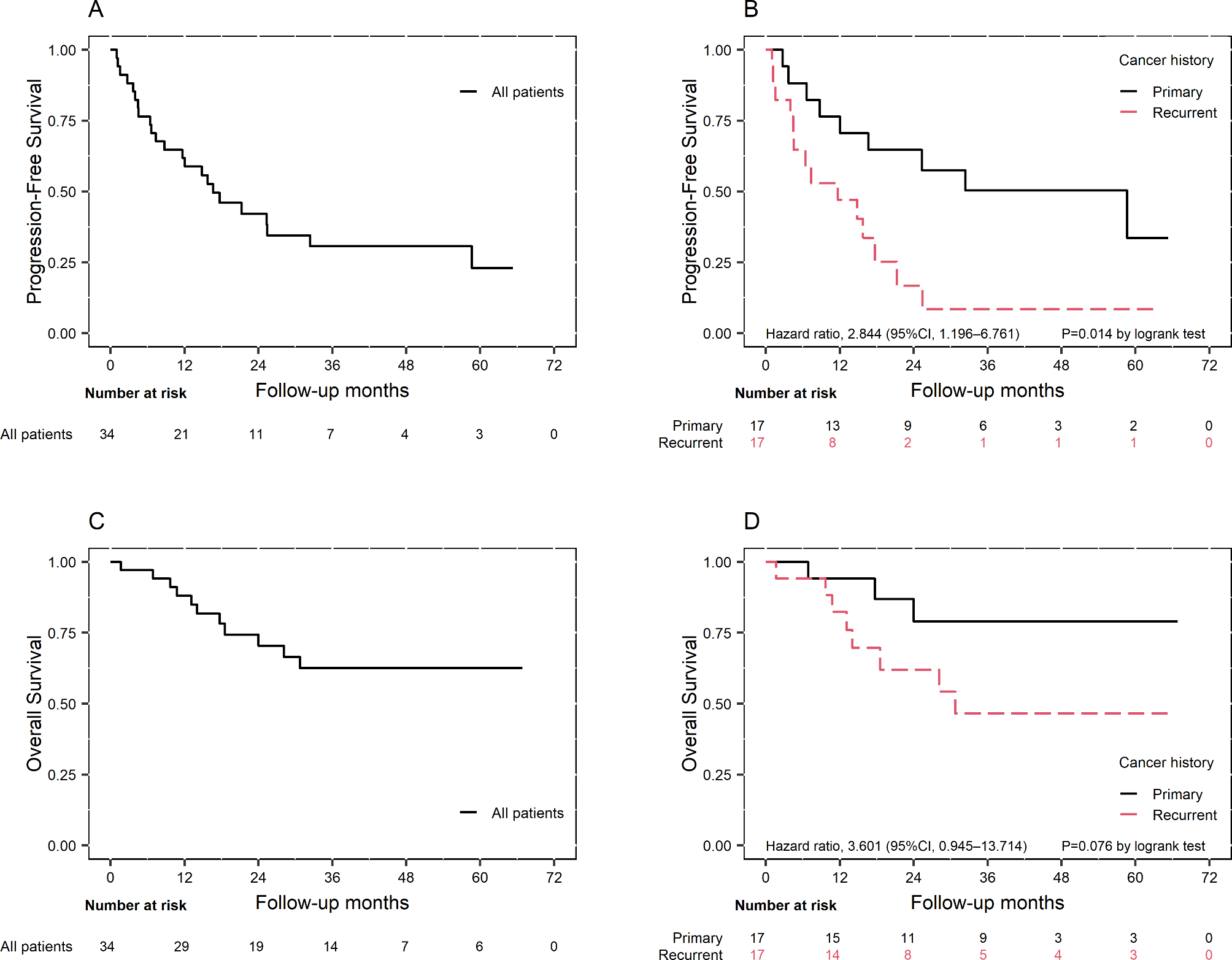
The patients’ characteristics were presented as mean with standard deviation (SD) and median with interquartile range (IQR) for continuous variables, and count with percentage for categorical variables. Survival curves for overall survival (OS) and PFS were estimated using the Kaplan-Meier method, and log-rank tests were used for comparisons based on disease status before CRS/HIPEC or expression levels of biomarkers.
Adjusted hazard ratios (HRs) were calculated using Cox proportional hazards regression, along with their corresponding 95% confidence intervals (CIs), to assess the association between each pre-/post-treatment or change in cytokine concentration and disease progression. Time to progression was defined as the number of days between the date of CRS/HIPEC and the date of recurrence, death, or the end of follow-up.
The regression models were adjusted for predetermined confounders, including age at CRS/HIPEC, pre-CRS/HIPEC body mass index (BMI), PCI, CC score, disease status before CRS/HIPEC (primary or recurrence), and FIGO stage at diagnosis. Associations between biomarkers and recurrence within 1 year and beyond 1 year post CRS/HIPEC were examined using interval-specific HRs (95% CIs). IHC expression was calculated by Wilcoxon Rank-Sum Test. Statistical analyses were performed using SAS 9.4 (SAS Inc., Cary, NC) and R 4.2.3 (R Foundation for Statistical Computing, Vienna, Austria) software. Given our sample size, we acknowledge potential biases that might affect our findings: selection bias due to the single-center nature of the study, and possible confounding bias despite our adjustment for known prognostic factors. These biases could impact our study conclusions by limiting the generalizability of our findings to broader patient populations. To minimize these potential biases, we utilized standardized laboratory procedures, and multivariate analyses adjusting for key clinical variables. All statistical tests were two-sided, and a P value < 0.05 was considered statistically significant.



留言 (0)