This systematic review demonstrates the efficacy of ADSCs in diabetic foot ulcers versus standard wound care methods in terms of total Healing State (Risk ratio = 1.56, 95% CI [1.32, 1.86], P < 0.00001) the primary efficacy outcome in most of the studies reviewed, Five studies showed that participants in the Adipose adipose-derived stem Cells (ADSCs) group had a significantly higher complete healing rate compared to the Standard care group, The homogeneity of the pooled studies (Chi square P = 0.48; I2 = 0%) suggests consistent results across different studies, reinforcing the association between ADSC therapy and an improved total healing state. Regarding healing rate, the overall effect estimate strongly favors the ADSCs group, with a pooled effect estimate of 1.84 (95% CI [1.51, 2.89], P < 0.00001). This consistency across studies (Chi square P = 0.75; I2 = 0%) highlights the reliability of the findings. Subgroup analysis further emphasizes the efficacy of ADSCs at different follow-up points (3 weeks, 4 weeks, 6 weeks, 2 months).
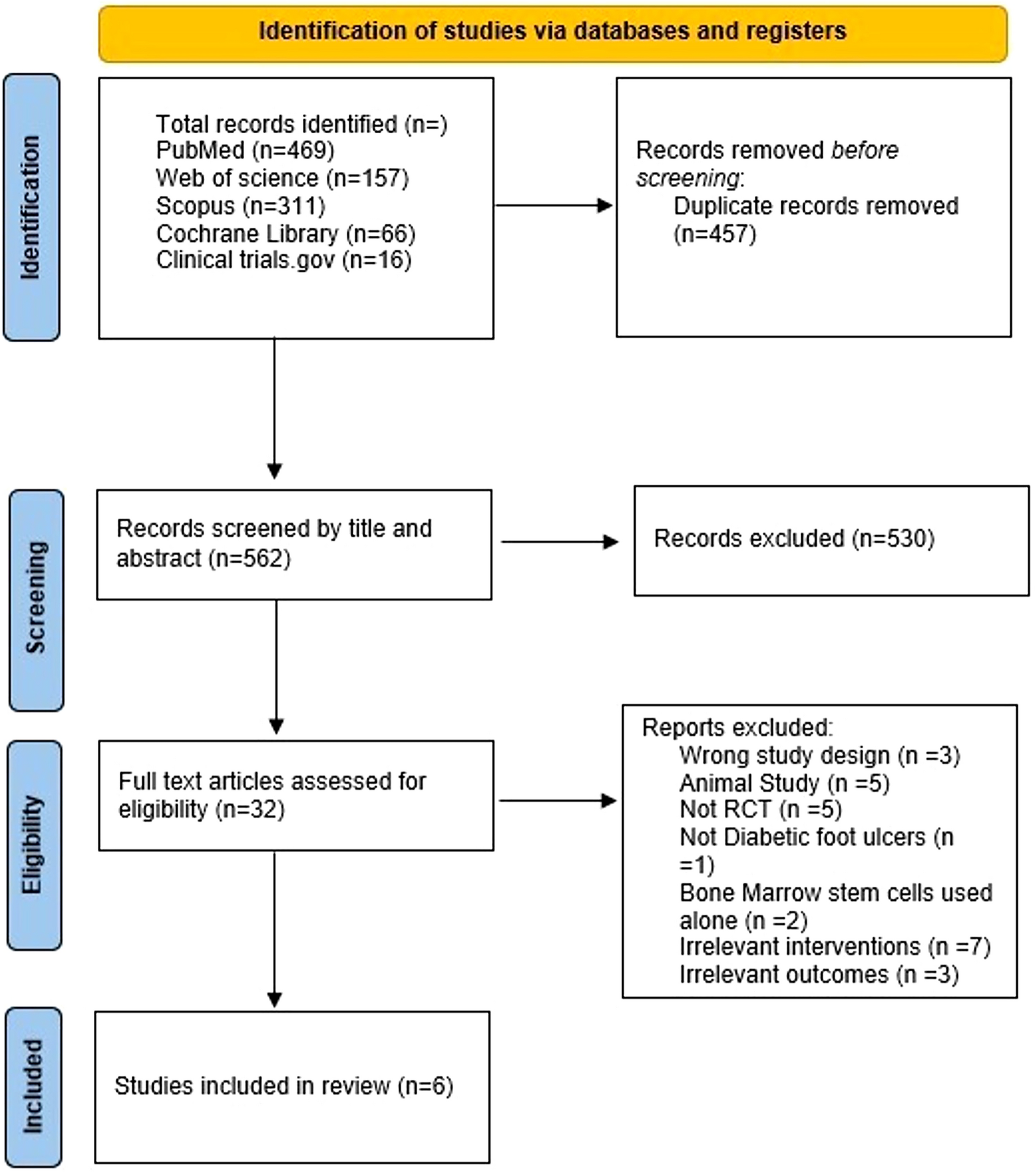
Among the studies we selected, 4 studies applied autologous ADSCs on 130 patients totally [17, 18, 21, 22] and the other 2 studies used allogenic ADSCs with a total population of 32 patients [19, 20].
Regrading ulcer size, (Thamm et al. 2020) reported significant wound reduction in favor of ADSCs group at weeks 2 and weeks 3 (P = 0.014), (P = 0.0004) respectively) but the final measure at 2 months was insignificant (p = 0.081) [21]. (Moon et al. 2019) reported higher wound size reduction for ADSCs than control group at week 1 (P = 0.007), it was also significant at week 9 and week 12 [20]. Smith et al. [20] report change of ulcer size between week 0 to week 12, the mean of Ulcer size decreased from 6.4 to 3.4 cm2 in the Control group and from 3.1 to 1.4 cm2 in the ADSCs group [22].
As regards wound infection [19, 20, 22], excluded patients with active wound infection or any systemic infection from the study [19, 20, 22], moreover Lonardi et al. [18] considered wound infection a failure of wound healing [18]. On the other hand, Tanios et al. [17] reported that 20 patients had an infected ulcer at the beginning of the study, 10 on each group, while at the end of the study only three (6%) patients in the study group developed infection, whereas 14 (28%) patients in the control group developed infections [17]. Thamm stated that 96.2% of population have bacterial colonization verified by wound swabs [21].
Regarding histological assessment, Thamm et al. [21] reported that neovascularization was observed higher in the group receiving ADSCS, Tanios et al. [17] reported a better re-epithelization and formation of granulation tissue in ADSCs group [17, 21]. In another clinical trial involving 16 patients aimed at investigating the therapeutic effect of fat graft in comparison to routine care and fat graft application with platelet rich plasma on DFUs reported that there was better angiogenesis in the fat graft group [23].
Regarding the safety, ADSCs were safe in our included studies except for minor adverse events as 2 abdominal hematomas as reported in Tanios et al. [17], wound infection as reported in Thamm et al. [21] and also Pain level was reported in 2 studies [18, 21] as visual analogue scale (VAS) (1–10) and in another one [19] it was as a part of Short Form (SF-36) score but all of them stated no significant difference between two arms [18, 19, 21, 24, 25]. none of the 2 studies [19, 20] used allogeneic ADSCs reported any adverse effects related to immune reactions.
Quality of life was reported on different scales in 2 studies. In Uzun et al. [19], it was reported through SF-36-Physical functioning and SF-36-General health resulting in significant difference in favor of ADSCs group (P = 0.017, P = 0.010, respectively) [24]. Smith et al. [22] used a health-related quality of life (HRQOL) questionnaire resulting in a significantly lower score for the control group (P < 0.05). Also, in another cohort study done on Lonardi et al. [18] subject, it was concluded that ADSCs achieve a better quality of life and decrease the length of hospital stay [26, 27].
Regarding cost effectiveness [22], stated that there is no significant difference between two groups [22]. While [19] reported that ADMSCs group costs more than control group (6695.3 ± 329.0 USD, 4082.0 ± 979.8 USD, respectively (P = 0.001) but it may be cost effective modality due to its benefits in achieving early return to work and decreasing recurrence and amputation rate [19].
Regarding our study, 6 clinical trials were included, reported that more participants healed completely by the end of follow-up duration in the ADSCs group compared with the Standard care group, and for the healing time, ADSCs groups showed significantly lower healing time than the standard care groups. In spite of the methodological and clinical heterogeneity observed in our 6 included studies, our meta-analysis assumed that ADSCs could be a promising option for treatment of DFU as the 6 studies reported more healed patients at the end of follow up duration and lower healing time for ADSCs group.
Our study’s findings showed that ADSCs groups have a better healing rate and lower healing time, in addition to better overall healing results than standard care groups confirming that ADSCs have an advantage over standard care groups. However, Several limitations must be considered first standard care for DFUs varied widely across studies, complicating comparisons. Lonardi [18] used sodium hypochlorite and saline solution with paraffin gauze, emphasizing rest and immobilization [18]. Moon [20] used hydrogen peroxide and saline with polyurethane foam [20]. Smith [22] followed individualized clinical guidelines, while Tanios [17] employed local anesthesia, debridement, and betadine ointment every 3 weeks [17, 22]. Thamm [21] used saline injections with polyurethane dressings, and Uzun [19] employed conventional glucose regulation and negative pressure therapy [19, 21]. This variability in standard care methods presents a limitation, as the lack of standardization in cleaning, dressing, and offloading protocols hinders the establishment of unified treatment guidelines Furthermore, our findings are limited by the small number of reported outcomes and there is other data like ulcer size reduction, pain level, cost effectiveness and other outcomes that cannot be assessed within our statistical analysis due to insufficient data provided in the selected studies, Significant heterogeneity was noted in the finding reported. Therefore, we performed subgroup analyses to determine the cause of heterogeneity. Our studies also have high risk of bias in some domains due to the presence of some concerns regarding selective reporting and blinding which is unavoidable in most surgical intervention studies. Therefore, our results should be cited with caution.

留言 (0)