
記住我



In this EGPA cohort, GI lesions were observed in 52 (31.5%) patients. Among the patients with GI manifestations, 22 developed severe GI disorder and the remaining 30 presented with relatively mild symptoms. The average age of EGPA patients was 45.3 ± 14.7 years and the ratio of male to female was 1.5:1 (98 males: 67 females). The median duration from the initial symptoms to EGPA diagnosis was 12 (IQR, 1–47) months, and the median duration from allergy to EGPA diagnosis was 25 (IQR, 2–74) months.
Clinical characteristics of GI involvement in patients with EGPAThe clinical characteristics of 22 patients with EGPA-related GI involvement in this cohort are summarized in Table 1. Furthermore, we reviewed the clinical features, treatment, and outcomes of patients with severe GI involvement in Table 2 to provide more details. The most common manifestations were abdominal pain (78%), diarrhea (40.4%), and nausea and/or vomiting (32.7%). Severe GI involvement mainly presented as upper and/or lower GI hemorrhages (14/52, 26.9%), ulcers (9/52, 17.3%), and obstructions (5/52, 9.6%). All five patients with obstruction had incomplete bowel obstruction, characterized by abdominal pain, reduced defecation and exhaust, and abdominal distension. Pancreatitis occurred in three patients with EGPA (5.8%), characterized by young age (26, 27, and 38 years old), and imaging showing that the pancreas was plump or diffusely enlarged. One patient experienced a recurrent attack of pancreatitis, which was considered chronic inflammation. Another patient was complicated with pancreatic pseudocyst, causing worsening abdominal pain. Through CT-guided percutaneous drainage of pseudocysts, his abdominal pain was alleviated and the amylase decreased to the normal range. GI perforation was observed in two patients with upper and lower GI involvement. Both patients were under 40 years of age, developed severe infections, and died within two months. The most common site of lesions was the upper GI tract including the stomach and duodenum, followed by the lower GI tract, which mainly included the small intestine and colorectum. Occasionally, the pancreas and gallbladder were affected.
Table 1 Characteristics of gastrointestinal involvement in EGPATable 2 Clinical features, treatment, and outcomes of EGPA patients with severe GI lesionsTwenty-eight patients with EGPA and GI lesions had post-operative pathology. Of these, twenty-three patients presented with chronic or acute inflammation of GI mucosa with eosinophilic infiltration, indicating eosinophilic gastroenteritis. A few patients showed lymphoid follicle formation or lymphocyte aggregation (six patients), inflammatory exudation (three patients), granulation tissue formation (one patient), or necrosis (one patient).
Comparison of clinical features between EGPA patients with and without GI lesionsGI-affected group had a significantly higher eosinophil ratio [32.0 (IQR 20.5–46.4) % vs. 23.5 (IQR 12.6–37.5) %, P = 0.016] than GI-unaffected group (Table 3). Compared to GI-unaffected group, GI-affected group had higher percentages of eosinophilic tissue infiltration (detected in any organs) (82.9% vs. 55.3%, P = 0.006), weight loss (55.8% vs. 32.7%, P = 0.005), and central nervous system (CNS) involvement (26.9% vs. 10.6%, P = 0.008). Fever, myalgia, and skin involvement were more common in GI-affected group than in GI-unaffected group; however, the differences were not significant (P > 0.05). Other clinical manifestations, demographics, and laboratory test results present no statistical differences between patients with and without GI lesions.
Table 3 Comparison of clinical features between EGPA patients with and without GI lesionsDisease activity and prognosis assessment at baselineAs shown in Table 3, the baseline disease activity in GI-affected group was higher than that in GI-unaffected group, as evaluated by median BVAS (18 vs. 14, P = 0.001). When we removed GI domain from the BVAS system, the two groups were comparable (16 vs. 14, P = 0.116). Regarding the prognosis assessment at baseline, the percentage of FFS ≥ 2 was higher in GI-affected group than in GI-unaffected group (32.7% vs. 9.7%, P < 0.001).
Stratified analysis of EGPA patients with GI lesionsPatients with GI lesions were stratified into two subgroups: patients with and without severe GI lesions (Table 4). The group with severe GI lesions had a shorter duration from the initial symptoms to EGPA diagnosis compared with the group without severe GI lesions [4 (IQR 1–18) versus 18 (IQR 7–60) months, P = 0.028]. Concerning laboratory examinations, higher trends were observed in erythrocyte sedimentation rate [44 (IQR 29–66) vs. 29 (IQR 6–45) mm/1h, P = 0.056] and C-reactive protein [39.5 (IQR 10.6–87.2) vs. 6.8 (IQR 2.0–40.7) mg/L, P = 0.053]. Notably, positive proteinase 3-ANCA results were only observed in severe GI-affected group (13.6% vs. 0%, P = 0.070). Regarding clinical manifestations, the group with severe GI lesions had less frequent severe asthma (45.5% vs. 76.7%, P = 0.021) and ear-nose-throat (ENT) involvement (45.5% vs. 80.0%, P = 0.010) than the group without severe GI lesions. The proportion of patients with CNS involvement was relatively higher in the severe GI-affected group (40.9% vs. 16.7%, P = 0.052), but the difference between the two groups did not reach statistical significance.
Table 4 Clinical features of EGPA patients with severe gastrointestinal lesionsIndependent factors associated with the development of GI lesions in patients with EGPAWe further analyzed independent factors associated with GI involvement in patients with EGPA using a multivariable logistic regression model (Fig. 1). Eosinophilic tissue infiltration (detected in any organs) (odds ratio [OR] 5.814, 95% confidence interval [CI] 1.747–19.344, P = 0.004), weight loss (OR 3.334, 95% CI 1.188–9.355, P = 0.022), and myalgia (OR 3.902, 95% CI 1.059–14.373, P = 0.041) were the significant factors associated with GI lesions in EGPA.
Fig. 1
Independent factors associated with gastrointestinal involvement in patients with EGPA. Multivariate logistic regression analysis was conducted for patients with gastrointestinal lesions in EGPA and the result is presented with the forest plot. CNS, central nervous system; EGPA, eosinophilic granulomatosis with polyangiitis; OR, odds ratio. Eosinophilic tissue infiltration refers to eosinophils infiltrating in any organs
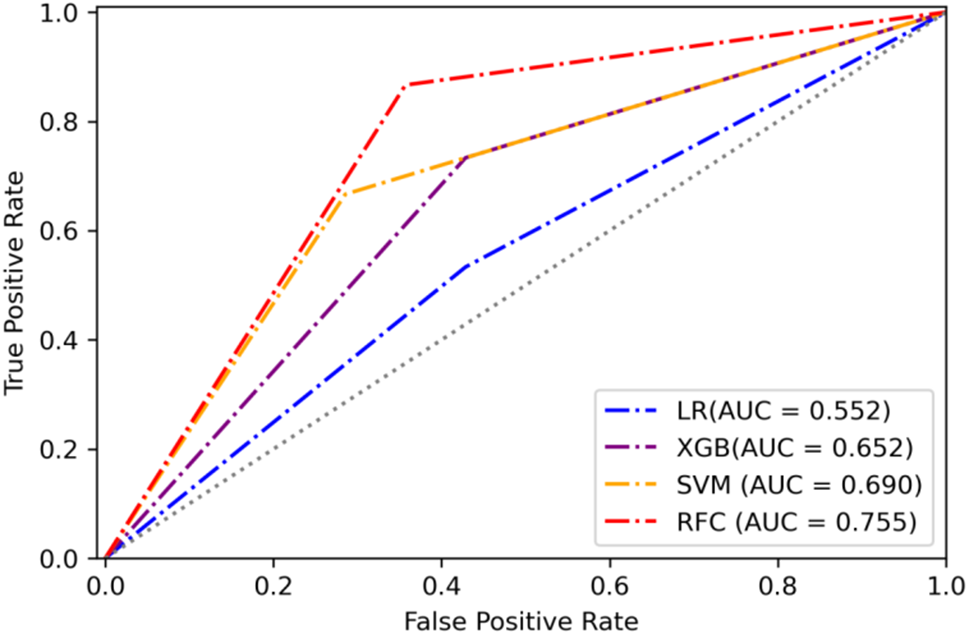
Prediction model and internal validationNext, we established a risk prediction model via a nomogram (Fig. 2A). The final model retained weight loss, CNS involvement, myalgia, and eosinophilic tissue infiltration (detected in any organs). Each item was assigned points according to its value, and the sum of all points was associated with the predicted probability of GI lesions. The C-index for this model was 0.772 (95% CI: 0.698–0.846), and the corrected C-index was 0.755. Internal validation of the model was performed using bootstrap. The calibration curve for 1000 bootstrap replications presents a comparison of the actual and predicted probabilities in Fig. 2B. To analyze the risk stratification produced by the final equation, we outlined the ROC curve to evaluate our model in Fig. 2C (AUC = 0.772).
Fig. 2
Prediction model performance and internal validation for GI lesions in patients with EGPA. (A) Nomogram predicting the probability of GI lesions in patients with EGPA. Points for weight loss, CNS lesions, myalgia, and Eos infiltration can be acquired using a point caliper and then summed to obtain a total score. (B) Calibration curve of GI lesions prediction model was obtained by comparing the observed and predicted risk of GI lesions in patients with EGPA. (C) Receiver operating characteristic curve of the GI lesions prediction model. AUC: area under the curve; CNS, central nervous system; EGPA, eosinophilic granulomatosis with polyangiitis; Eos_infiltration, eosinophilic tissue infiltration (detected in any organs); GI, gastrointestinal
Eosinophils were an important parameter in assessing disease activity and predicting GI lesionsBased on the above analysis in Table 3, we found that the eosinophil ratio was significantly higher in the GI-affected group, and the eosinophilic tissue infiltration (detected in any organs) was the most significant independent factor associated with GI lesions in patients with EGPA. We further performed the correlation analysis between the circulating eosinophils and BVAS at baseline (Fig. 3A and B) and found that both the eosinophil ratio (r = 0.160, P = 0.045) and eosinophil count (r = 0.233, P = 0.004) in blood were positively correlated with BVAS at baseline. In addition, the cutoff value of the circulating eosinophil ratio was calculated to identify the GI lesions in patients with EGPA (Fig. 3C). The optimum cutoff value of the eosinophil ratio was 19.2% with a sensitivity of 82.0% and a specificity of 41.7% (area under the curve = 0.62, P = 0.0098).
Fig. 3
Eosinophils were an important parameter to assess disease activity and predict GI lesions in EGPA. Correlation of BVAS with eosinophil ratio (A) and count (B). Pearson correlation was calibrated for the analysis. (C) Receiver operating characteristic curve of eosinophil ratio for identifying patients with GI lesions in EGPA. AUC: area under the curve; BVAS, Birmingham Vasculitis Activity Score; EGPA, eosinophilic granulomatosis with polyangiitis; EOS, eosinophil; GI, gastrointestinal
Identification of clinical patterns of EGPA based on phenotype clustersFive clinical patterns were identified using correlation matrix analysis (Fig. 4). “Brain-gut pattern” was well-defined based on an association between CNS lesions and GI involvement. “Joint-muscle-skin pattern” can be found in the figure, where arthritis, myalgia, and skin involvement show a close link. Cardiac manifestations were separately identified as a unique pattern on the cluster panel of EGPA (Cardiac pattern). “Respiratory pattern” was constructed based on the association between asthma and ear-nose-throat involvement. “Renal-peripheral nervous system pattern” was observed as the fifth pattern, characterized with an association between renal and peripheral nervous system involvement.
Fig. 4
Correlation analysis of different organ involvement. Spearman’s correlation coefficient is utilized to assess the correlation between two variables. A coefficient value approaching 1 signifies a stronger positive correlation, a value approaching − 1 indicates a stronger negative correlation and a value approaching 0 indicates a weak correlation. CNS, central nervous system; ENT, ear-nose-throat; PNS, peripheral nervous system
Treatment and outcomesThe induction therapies used in this cohort were GCs and immunosuppressants, with CYC as the primary immunosuppressive agent. MP pulse was administered more frequently in patients with severe GI involvement than in patients without severe GI involvement (50.0% vs. 16.7%, P = 0.010; Table 4). The median follow-up duration was 23 months (range 1–120 months). Overall, there was no significant difference in the outcomes between GI-affected and GI-unaffected groups (P = 0.414; Fig. 5A). The all-cause mortality rate was 8% (4/52) in GI-affected group and 4% (5/112) in GI-unaffected group. Of the four deaths in GI-affected group, two patients had severe GI lesions including perforation and bleeding, one with cerebral hemorrhage, and the other patient died from septic shock and multiple organs failure. Moreover, the cumulative survival was comparable between the two groups, although it tended to be lower in GI-affected group (log-rank test, P = 0.429; Fig. 5B).
Fig. 5
Outcomes and survival of patients with EGPA with GI involvement. (A) Comparison of outcomes between patients with and without GI involvement in this EGPA cohort. (B) Comparison of cumulative survival rates between patients with and without GI involvement. CR, complete remission; EGPA, eosinophilic granulomatosis with polyangiitis; GI, gastrointestinal; PR, partial relief
留言 (0)