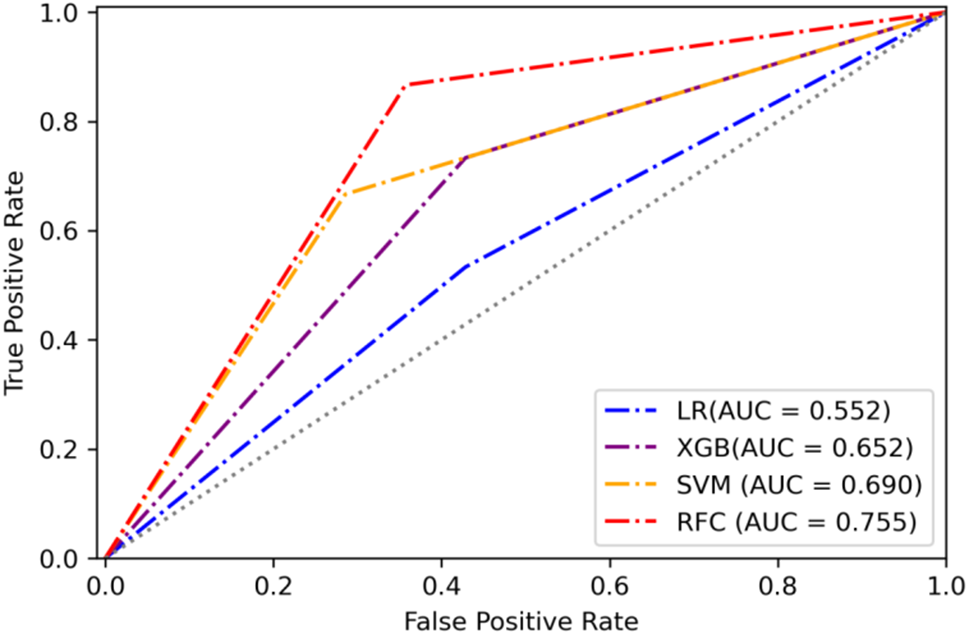
In this study, 96 patients diagonosed pSS were enrolled and analyzed to identify the predictors for AIT. We collected 14 demographic and clinical characteristics to identify the predictors for AIT. We created a random forest classifier, which is a part of machine learning, providing a more accurate prediction for the risk of AIT (AUC = 0.755) than logistic regression model (AUC = 0.552). In our study, AUC and ROC curves confirmed that the RFC model, based on predictors per our findings, had greater predictive efficiency than LR model, was widely reported in other disciplines as well [13, 14].
Autoimmune diseases affect approximately one in ten individuals [15]. There may be common pathogenesis or predisposing factors between different autoimmune diseases, especially between connective tissue diseases and endocrine diseases. pSS, one of chronic autoimmune diseases, was characterized by lymphocyte infiltration and specific autoantibodies. The most common thyroid disorders of pSS are autoimmune thyroiditis, mainly caused by TPOAb and TgAb [16]. Therefore, in this paper, the detection of TPOAb and TgAb was used as an objective index to evaluate AIT.
Age, IgG, C4, and dryness of mouth, were the top four most important characteristics. In our series, age accounted for the largest proportion of the feature weight. As known, the peak prevalence of pSS and AIT occurs between 30 and 50 years in both. Previous studies found that the peak age of onset in pSS with AITD patients ranges 45 to 54 years old, consistent with our study [17]. The patients of pSS with AIT are younger than those without AIT, in agreement with others [18]. So younger patients with pSS should pay more attention to the possibility of autoimmune thyroiditis.
B-cell hyperactivity is a hallmark of pSS [19]. Hyperglobulinemia is one of the most common clinical manifestations of B cell hyperactivity. Significant serum immunological features in pSS patients were hyperglobulinemia and positive for multiple autoantibodies, such as anti-SSA, anti-SSB and ANA. Previous researches proved that more than 70% of pSS patients have elevated serum IgG levels [20]. Recent studies showed that hyperimmunoglobulinemia can indeed increase death and important damage to the renal, pulmonary, interstitial, haematological or neurological involvement [21,22,23]. In our study, elevated level or normal range but close to upper limit IgG levels were observed in both group. However, the group of pSS with TPOAb and TgAb presented lower levels of IgG than those without. IgG is classified into four subclasses, IgG1 to IgG4. Previous studies have indicated that.
IgG1 and IgG4 are mainly elevated in AIT patients, and IgG1 and IgG3 are mainly in pSS [24, 25]. Despite the high degree of homology in the amino acid sequence of IgG subtypes, they have unique characteristics in binding antigens, activating complement, triggering effect cells, and tissue distribution. In several studies recently, immunohistochemistry has indicated numerous IgG4-positive plasma cells in a fraction of HT [26, 27]. Another study showed that IgG4 HT, grouped based on immunostaining results of thyroid, had higher levels of thyroid autoantibodies compared to those classified as non-IgG4 positive [28]. These findings indicate that the IgG4 subtype of AIT is prone to deposit and destroy thyroid cells in endocrine gland tissue. Therefore, although serum IgG levels in pSS patients with AIT do not appear to be higher, there may be a specific IgG subtype that is more readily distributed to the affected glands. Regrettably, our study did not investigate the distribution of IgG subtypes and IgG deposition in the affected tissues of patients with positive thyroid autoantibodies, which may be an important research direction for the future. We hope future studies can better answer this question.
In addition, we found that C4 levels of pSS with TPOAb or TgAb are lower. The same results was found in pSS with HT [18]. The results of this study showed that pSS-AIT patients had lower C4 levels. In a large cohort of 921 Spanish patients with pSS, reduced C3 and C4 complement fractions at the pSS diagnosis was observed and this finding was associated with disease activity [29]. Hypocomplementaemia was detected in 24% of patients with pSS and low C4 level was also closely associated with the two main adverse outcomes of lymphoma development and death [30]. Another survey of 723 patients with pSS found that low levels of C4 and obvious purpura were the most threatening risk factors for lymphoma after 6 years follow-up [31]. High titer TPOAb is one of the main causes of AIT. The mechanism is that TPOAb destroys thyroid tissue through antibody-dependent cytotoxicity and complement-dependent cytotoxicity, leading to reduction of complement components. This implies that high titer thyroid autoantibodies in pSS patients may activate complement-dependent cytotoxicity leading to high disease activity or multiple organ dysfunction, and even lymphoma.
In our study, no symptom of dry mouth is a risk factor for developing pSS with AIT. From the analysis of 100 Italian patients affected by pSS, it was similarly found that pSS associated with HT, a common subtype of AIT, complained less frequently of xerostomia [18]. A cross-sectional study included 305 subjects with sicca symptoms showed that high prevalence of AIT in subjects with sicca symptoms, especially mouth dryness [4]. In this study, AIT precedes SS in only 13% of patients. In 50% of patients, the diagnosis of HT was secondary to pSS after a mean follow-up of 5.5 years [17]. It means that symptoms of eyes or mouth dryness should be seriously considered as a possible symptom of SS, as well as AIT (sometimes both). Therefore, we need to actively screen thyroid function and thyroid autoantibodies in the initial diagnosis of pSS and subsequent follow-up.
Our study is not without limitations. First, retrospective design limits our ability to draw causal inferences from the associations found. The sample size, while adequate for initial explorations, is relatively small for generalizing the findings across diverse populations. Second, this study lacks the collection of thyroid ultrasound data. The absence of TPOAb and TgAb in some AIT patients may be helpful in the diagnosis based on the ultrasound features of the thyroid gland. Thirdly, our study did not explore the distribution of serum IgG subtypes and the deposition of IgG subtypes in thyroid glands. Future studies should aim to include a larger cohort to validate these predictors and potentially uncover new ones.




留言 (0)