The aims of the present study were to assess the proportion of confirmed LNB among patients with clinically suspected early LNB, and to evaluate and compare the proportion of confirmed LNB for three different clinical presentations, i.e., for patients who present with radicular pain of new onset, for those with PFP and/or involvement of another cranial nerve without radicular pain, and for those with EM associated with symptoms suggestive of nervous system involvement but without either radicular pain or cranial nerve palsy. We chose these three groups to evaluate because they represent the most common clinical manifestations of LNB in adult patients in Europe [3, 16].
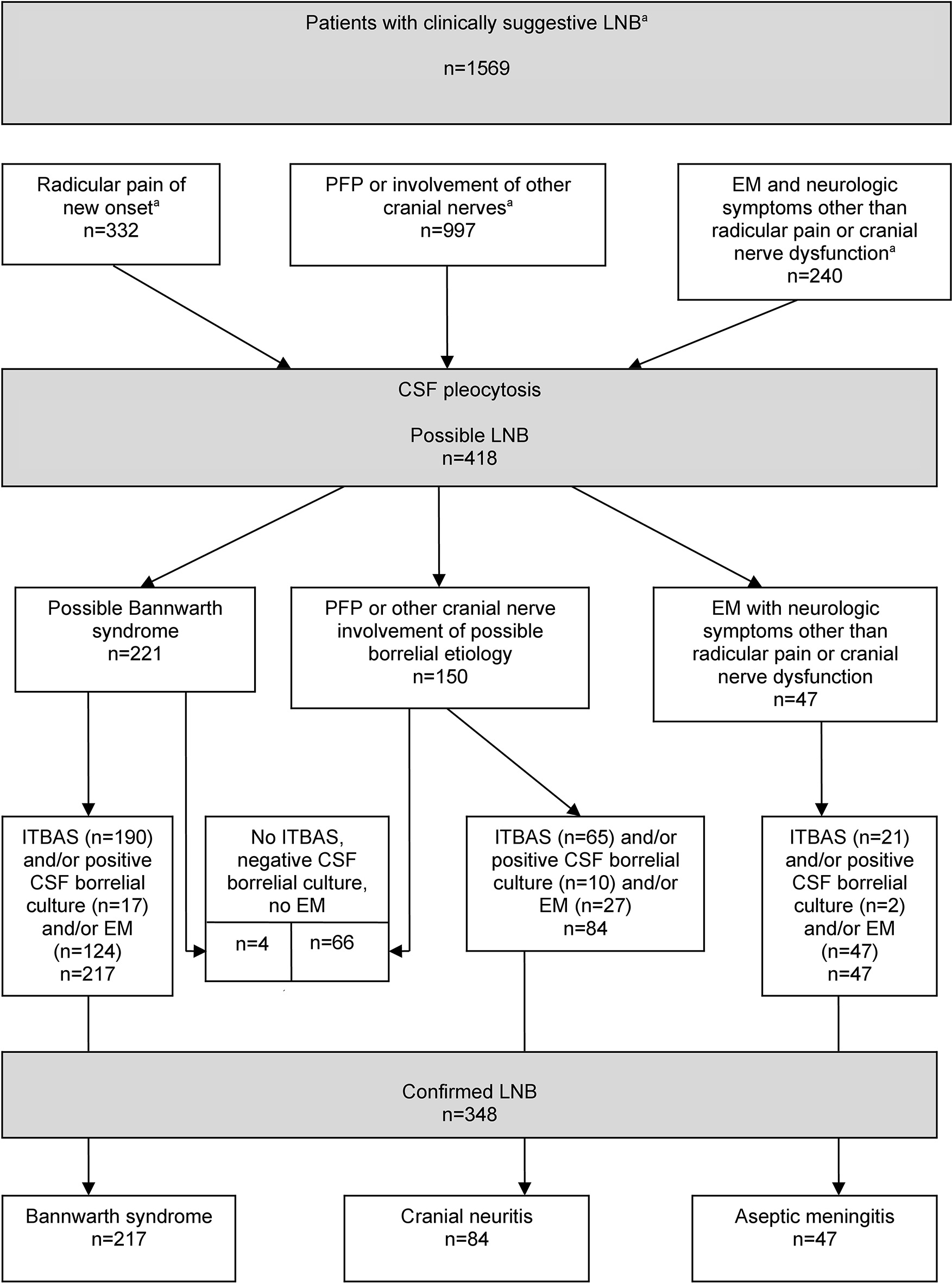
The analysis used in the current study was based on the same reasoning that is used in everyday clinical practice for patients with a reasonable clinical suspicion of LNB and without an obvious other cause of a nervous system illness. Since the diagnosis of LNB in accordance with the European Federation of Neurological Societies (EFNS) criteria [17] requires a CSF examination, and since basic CSF results (leukocyte count) are available relatively quickly (in < 1 h) and much earlier than the results of serologic tests for Borrelia or the results of Borrelia cultures, we used the corresponding “natural clinical” sequence as shown in the Fig. 1: (1) Clinical suspicion of LNB without an obvious other cause of nervous system illness; (2) Confirmation of inflammation of the central nervous system (i.e., demonstration of CSF pleocytosis); and (3) Evidence indicating that the inflammation is most likely caused by Borrelia.
The main findings of the present study were the pronounced differences in the probability for confirmed LNB among the different presentations of clinically suspected LNB evaluated. The majority (63.5%) of the 1569 patients from Slovenia evaluated in this study presented with PFP and/or involvement of another cranial nerve without radicular pain, 21.2% had radicular pain of new onset, while 15.3% had EM and neurologic symptoms without radicular pain or cranial nerve palsy. Of these 1569 patients, 348 (22.2%) fulfilled the criteria for confirmed LNB: 217 had Bannwarth syndrome, 84 had cranial neuritis with CSF pleocytosis and 47 had CSF pleocytosis with EM but without radicular pain or cranial neuritis. Although these findings corroborate previous reports that Bannwarth syndrome is the most frequent manifestation of early European LNB in adults [6, 18,19,20], it should be mentioned that in the present study, patients were predominantly referred to us by primary care physicians. Although the large majority of patients with suspected LNB are referred to our LB Outpatient Clinic and only a few instead to neurologists, the proportions of referred patients with individual clinical manifestations might differ from the proportions of LNB clinical manifestations in other health care settings.
Our study demonstrated that the proportion of confirmed early LNB substantively differed when comparing three distinct clinical presentations. Although among patients referred for suspected LNB those with cranial nerve involvement were the most common, in the group with confirmed LNB the number of patients with Bannwarth syndrome (clinically characterized with radicular pain) was higher than for those who presented with cranial neuritis, and also higher than for those who had EM associated neurologic symptoms and CSF pleocytosis but without cranial neuritis and/or radicular pain (aseptic meningitis). The reason for this was the different proportions of confirmed LNB among the 3 clinically suspected LNB groups: the proportion was highest in the group with new onset of radicular pain (217/332, 65.4%), which was 6.1-times higher than in patients without radicular pain (131/1237, 10.6%; p < 0.001) - i.e., 3.3-times higher compared to the group with EM associated neurologic symptoms but without cranial neuritis and/or radicular pain (47/240, 19.6%; p < 0.001), and 7.8-times higher than in patients with cranial neuritis (84/997, 8.4%; p < 0.001).
Of the 1569 patients evaluated, 348 (22.2%) fulfilled the criteria for confirmed LNB, whereas 1221 did not. Of the 1221 patients who did not meet criteria for confirmed LNB, 1151 (94.3%) patients had a normal CSF leukocyte count, while 70 (5.7%) patients had CSF pleocytosis but did not fulfill at least one of the three requirements for proof of Borrelia infection (ITBAS, isolation of borrelia from CSF, or the presence of EM). The latter group of 70 patients comprised four patients with new onset of radicular pain, and 66 patients with cranial neuritis without radicular pain. The fraction of patients who had CSF pleocytosis but did not fulfill at least one of the three criteria to confirm LNB was 4 of 221 (1.8%) patients with radicular pain, 66 of 150 (44%) patients with cranial neuritis without radicular pain, and none of 47 EM patients with neurologic symptoms other than radicular pain or cranial nerve involvement (this finding for the latter subgroup is obviously expected since EM was an inclusion criterion) (Fig. 1). Thus, the finding of CSF pleocytosis in a patient with radicular pain of new onset indicates a very high probability for confirmed LNB, while the presence of CSF pleocytosis in a patient with cranial nerve involvement has a much lower probability for confirmed LNB, based on the criteria used in this study. It is important to note that lack of confirmation based on the criteria used in this study does not exclude the diagnosis of LNB. Of interest, but not surprisingly according to some European reports on LNB [21,22,23], the likelihood of a diagnosis of confirmed LNB was associated with month of onset of the clinical illness. Onset in the 6-month period from May through October was statistically significantly higher for confirmed LNB compared with possible LNB cases, p < 0.001. The more even distribution of disease onset by month in patients with possible LNB indicates a less close temporal association with tick bites and suggests that this group likely includes persons without LNB.
Key strengths of our research approach are the large cohorts of well-defined patients with distinct clinical presentations suggestive of early LNB; the origin of patients from the same geographic region that enables an identical LB epidemiologic pattern for different clinical presentations; a comprehensive and standardized diagnostic approach over the 17 year study period, and an evaluation for all patients that included a clinical examination, an examination of CSF, a calculation of ITBAS, and a Borrelia culture of CSF (culture was performed in 397 of the 418 (95%) possible LNB cases); and the use of standardized LNB case definitions. In addition, the month of onset of symptoms was evaluated.
However, in addition to a potential referral bias, a limitation of this study is that it is based on patients at least 15 years of age and thus the findings, although relevant, may not be completely applicable to children. Moreover, although we believe that our findings are relevant to the other European regions endemic for LB, it is not clear how such findings may relate to patients with LNB in North America, where the disease is almost exclusively due to the borrelial species B. burgdorferi, and borrelial meningoradiculoneuritis is rare [24,25,26]. Another limitation of our study is that CSF Borrelia culture was only performed for 95% of the patients. Culturing B. burgdorferi s.l. from CSF has low sensitivity (in the present study Borrelia was isolated from CSF from only 29/397 (7.3%) patients with CSF pleocytosis), is a test that is not usually available to clinicians, and requires a considerable work-burden with a substantial delay in getting the test results. However, culture positivity is highly specific and offers the opportunity for genetic analysis of the recovered isolates of B. burgdorferi s.l. Of potential relevance, PCR for detection of Borrelia in CSF was not performed; PCR testing is not part of routine testing for LNB at our institution, since it has a relatively low sensitivity on CSF samples [27, 28].
However, future studies might consider adding PCR testing. In addition, testing for other pathogens that cause CSF pleocytosis besides TBEV (e.g., Herpes simplex virus (HSV), varicella zoster virus (VZV), enteroviruses, and Treponema pallidum) and for other epidemiologically relevant tick-transmitted microorganisms that may cause disease in humans (e.g., Anaplasma phagocytophilum, Borrelia miyamotoi, Neoehrlichia mikurensis, and rickettsiae) was not done. However, a study on the infectious etiology of peripheral facial palsy performed in the same geographical region revealed that likelihood of finding an etiology other than Borrelia was negligible: for example, of 364 patients for whom molecular testing for HSV-1, HSV-2, and VZV DNA was performed in CSF, none tested positive for HSV-1, none for HSV-2, and only 1 for VZV DNA [29]. Similarly, a study from the same geographical region (central Slovenia) revealed that in patients with EM associated with leukopenia and/or thrombocytopenia, Anaplasma phagocytophilum co-infections are rare [30].
Another study limitation is that newer laboratory diagnostic markers for LNB (such as measuring CXCL13 in CSF) were not used systematically throughout the time period evaluated and consequently were not included in the present report. The inclusion of CXCL13 as a diagnostic criterion might have resulted in detection of some additional LNB cases, especially in the group characterized with cranial nerve involvement.
In conclusion, although in our study nearly 3-times more patients with cranial neuritis than patients with radicular pain of new onset were included, the study findings corroborated previous reports that in a LB endemic region in Europe, such as Slovenia, borrelial meningoradiculoneuritis (Bannwarth syndrome) is the most frequent clinical manifestation of early LNB in adult patients [6, 18,19,20]. The main reasons for this finding were the pronounced differences in the probability for confirmed LNB among the different presentations of clinically suspected LNB. Patients with suspected LNB who presented with a new onset of radicular pain had a high (65%) probability for confirmed LNB, while the corresponding probability was more than 6-times lower for those who presented without radicular pain. Also as shown in this study, seasonality is also a pertinent variable in terms of the likelihood of diagnosing confirmed cases of LNB.



留言 (0)