In this monocentric retrospective study, we analyzed the risk factors and outcomes of adult hematological patients with BSI due to P. aeruginosa (PABSI) over nearly ten years. We found that antibiotic drug resistance is a main risk factor for increased mortality, most likely due to inadequate empirical therapy. The inadequacy of antibiotic therapy and the development of antibiotic resistance have been identified as risk factors for a fatal outcome in neutropenic patients with sepsis in previous studies [19]. These observations are consistent with those of other studies about PABSI caused by multidrug-resistant, sometimes hypervirulent isolates of P. aeruginosa in hematologic patients [20,21,22]. BSIs due to P. aeruginosa are associated with high rates of morbidity and mortality, with estimated mortality rates of 21–38% [6], which is in line with the observed mortality rate of 22% in our cohort [2, 19, 23]. Mortality is significantly higher in the presence of septic shock, in our cohort it was 100%, while another multicentric study showed a mortality rate of 75% [19]. We could confirm septic shock as a risk factor for mortality as demonstrated before [19]. In our cohort, as in other studies, previous antibiotic exposure was associated with occurrence of resistant P. aeruginosa [20, 24]. Of note, carbapenem exposure was associated with both carbapenem-resistance and fluoroquinolone-resistance in P. aeruginosa. Fluoroquinolone exposure was associated with both, cephalosporin-resistance and piperacillin/tazobactam resistance, whereas the association with fluoroquinolone-resistance remained at the margin of significance. We found higher rates of co-resistance compared to other studies [25]. P. aeruginosa has numerous intrinsic resistance mechanisms such as porin loss, efflux pumps and inactivating enzymes. It can also acquire resistance mechanisms, e.g. through mutation or horizontal gene transfer (e.g. metallo-betalactamases) [26]. The mechanism cannot be deduced from the resistance phenotype and since our strains were not available for whole genome sequencing, the causes for the observed resistance remain speculative.
It has been demonstrated that in patients with leukemia, the pathogen responsible for the BSI frequently dominates or colonizes the microbiota of the gastrointestinal (GI) tract [27]. In our hematology ward screening for MDR microorganisms is part of the institutional protocol. Conversely, preventing colonization, especially by MDR P. aeruginosa, could potentially reduce the risk of invasive infection. This could be achieved through antibiotic stewardship (AMS) measures to reduce selection pressure, supported by good hygienemanagement. AMS can help to reduce antibiotic exposure, e.g. by following guidelines, targeted therapy changes, shortening the duration of therapy and reducing fluoroquinolone prophylaxis (FQP) to a few high-risk constellations.
As about 60% of leukemia patients develop neutropenic fever and the prompt initiation of an empirical and Pseudomonas-active therapy, also depending on the local epidemiology, is strongly recommended. From 2013 to 2019, 308 BSI episodes occurred in hematological patients in our hospital. Neutropenic fever was present in 209 cases (68%). Gram-positive pathogens were detected in 53%, 41% of which were coagulase-negative staphylococci, corresponding to 22% of total detections. Gram-negative pathogens were identified in 47% of the cases, 12% of which were P. aeruginosa, corresponding to 6% of the total number of cases [28].
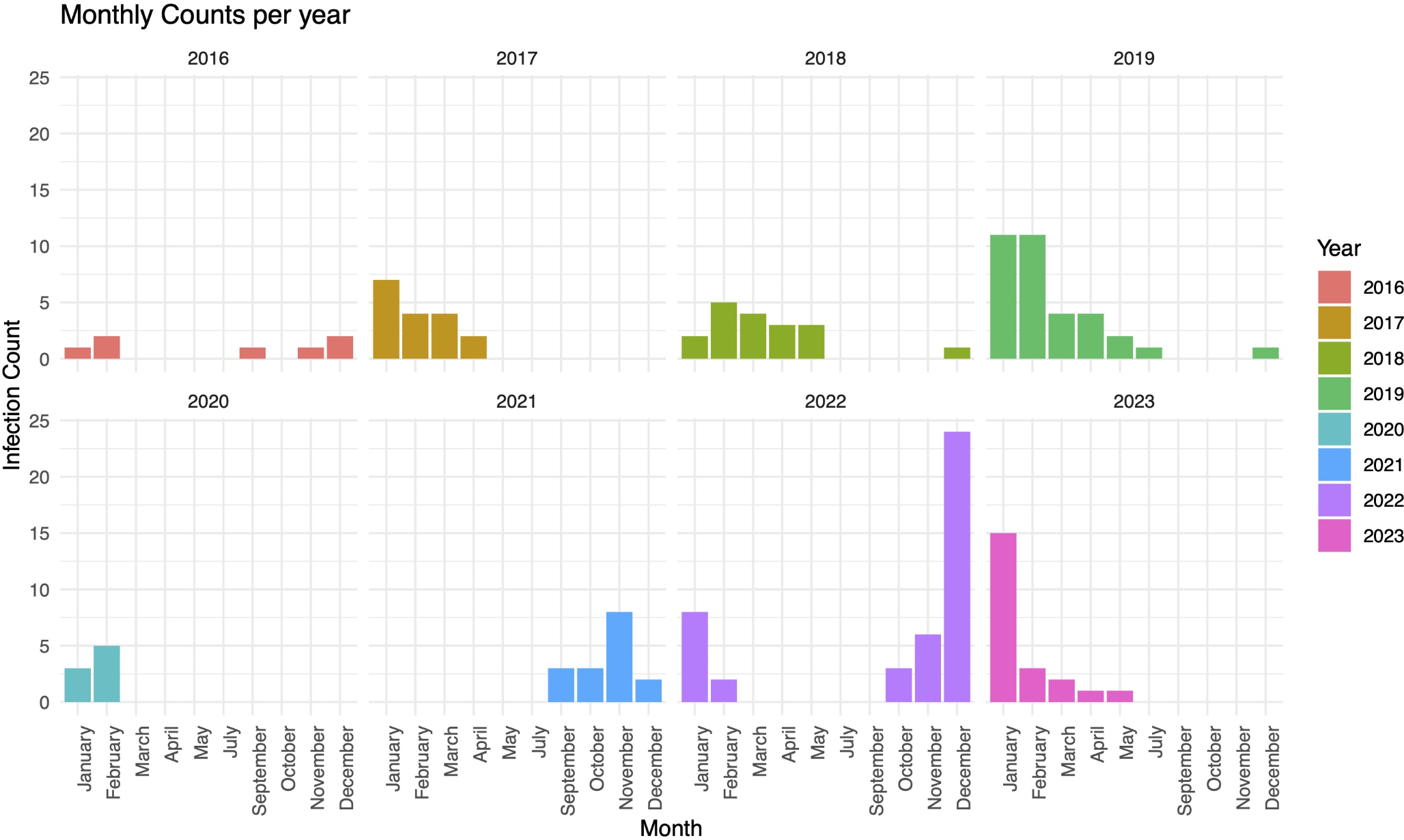
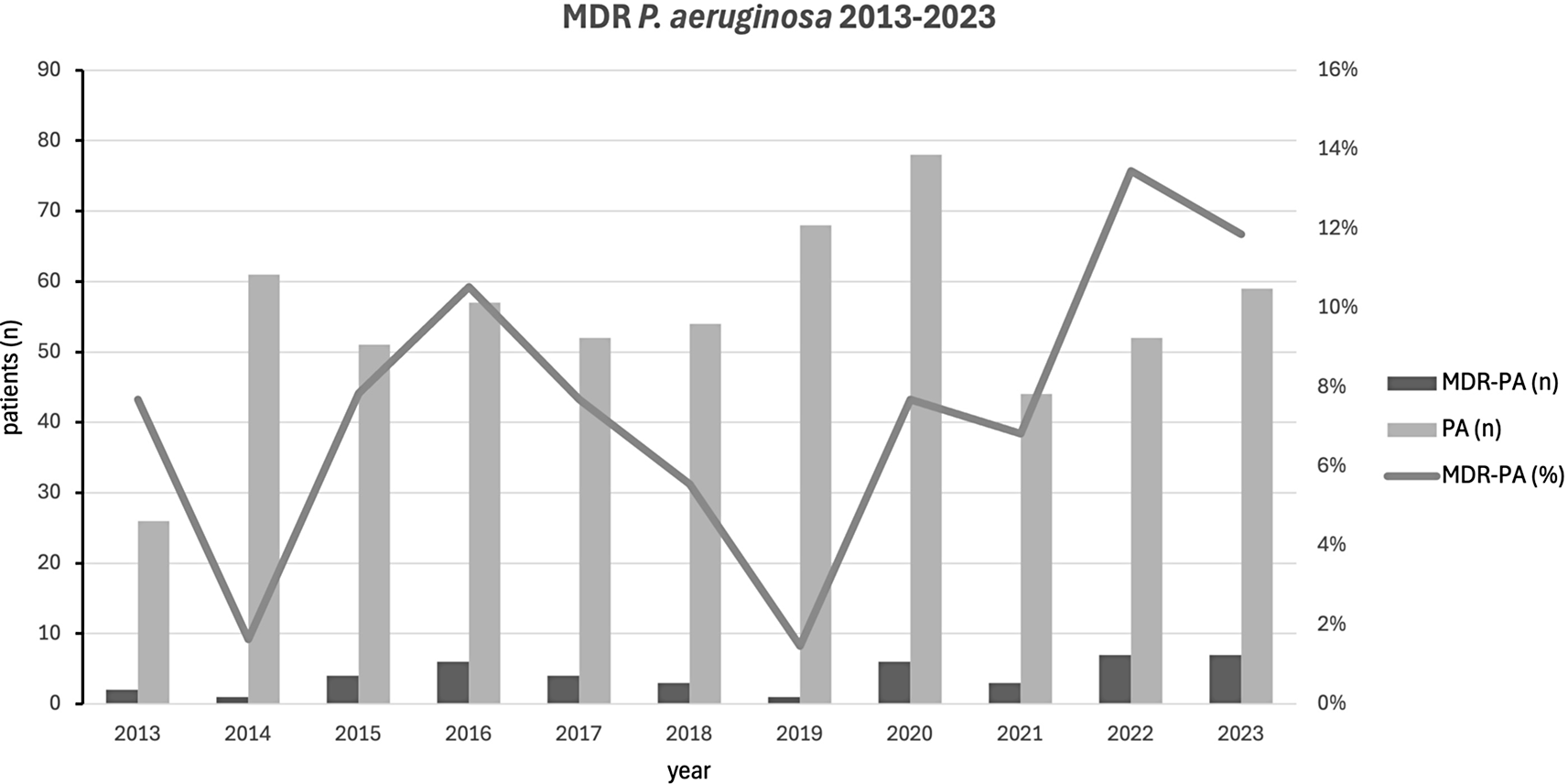
During 2013–2023 the rate of blood cultures positive for gram-positive organisms per year ranged from 54 to 75.2%, that of gram-negative organisms from 17,6% to 35,9%. The rate of P. aeruginosa positive blood cultures per year ranged from 1.7% to 9,8% corresponding finally to 50 patients having P. aeruginosa BSI. Of note, frequency of MDR P. aeruginosa at our hematology ward increased in the last years.
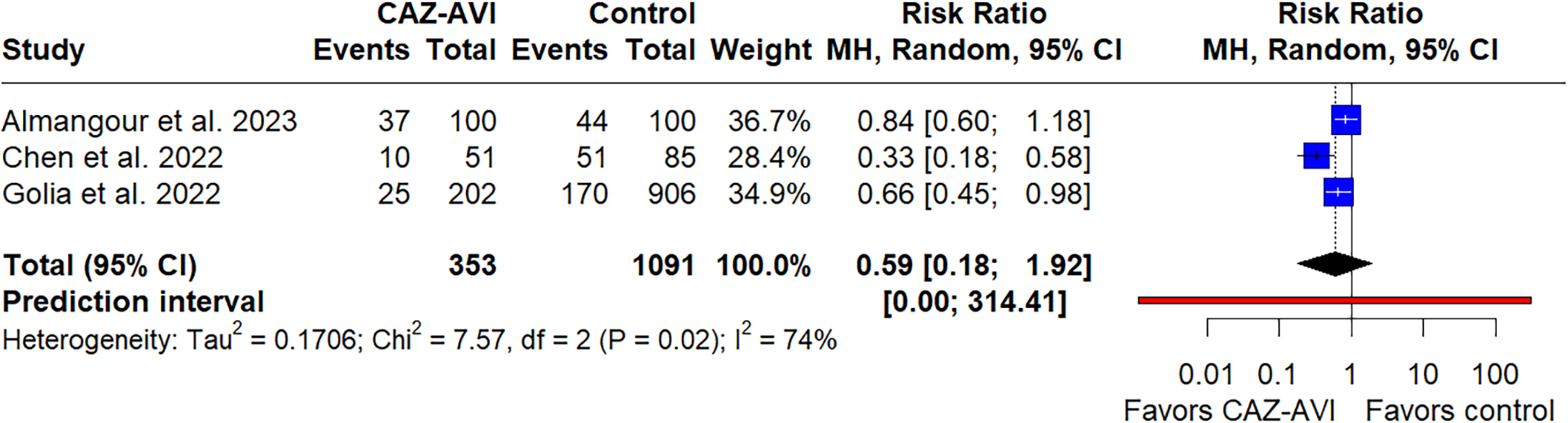
Most patients are extensively exposed to antibiotics and antibiotic selection pressure is a relevant problem [4, 29]. To minimize selection pressure and damage to the microbiota, antibiotic therapies should be prescribed for as long as necessary, but as short as possible. By deciding in favor of monotherapy versus combination therapy and a rational duration of treatment, antibiotic usage and thus selection pressure can be reduced. The superiority of combination therapy over monotherapy in PABSI is a subject of ongoing controversy. A meta-analysis showed no difference in terms of mortality, although data on infections with antibiotic resistant P. aeruginosa-BSI are scarce. For this reason, the current ESCMID guidelines do not include a recommendation for or against targeted combination therapy for infections caused by carbapenem-resistant P. aeruginosa [30]. In severe infections (sepsis), a combination is recommended, if monotherapy is based on either fosfomycin, a polymyxin or an aminoglycoside [30]. In line with this, the IDSA does not recommend combination therapy for PABSI, if one of the new beta-lactam/beta-lactamase inhibitor combinations (ceftazidime/avibactam, ceftolozane/tazobactam, imipenem/relebactam) or cefiderocol have been tested susceptible [31]. Current AGIHO guidelines strongly recommend the use of single-agent broad-spectrum Pseudomonas-active antibiotics such as piperacillin/tazobactam, ceftazidime, cefepime, meropenem or imipenem/cilastatin as first line antibiotic therapy [32]. However, in our cohort, 32% of patients received an empirical combination therapy, due to local treatment policy. With regard to the duration of therapy, it has been shown that the duration of treatment for febrile neutropenia, which is often determined by the time of regeneration, can be shortened in view of a 72 h fever-free status and clinical response, without any negative impact on clinical outcome [33]. Furthermore, a multicenter-study in onco-hematology patients with PABSI showed, that short-courses (7–11 days) of therapy were non-inferior in terms of clinical outcomes compared to prolonged courses (12-21days) [34].
The benefits of FQP have also been the subject of controversial debate for years. In the meantime, it has been repeatedly demonstrated that, although the omission of an FQP is associated with an increase in BSI, it is not associated with increased mortality [35, 36].
The effects of FQP on resistance selection were shown not only for P. aeruginosa infections, but also for both viridans streptococci and Enterobacterales [37] which in turn leads to reduced effectiveness of prophylaxis [38]. The empirical use of fluoroquinolones for combination therapy in neutropenic patients with sepsis can therefore not be recommended in centers where FQP is widely used or if colonization with a FQ-R pathogen such as P. aeruginosa or Enterobacterales is documented.
These observations compelled other centers to leave the FQP [39, 40]. Discontinuation of FQP has been shown to decrease FQ-R and 3rd generation cephalosporin resistance due to ESBL-producing Enterobacterales, without the increase of serious infectious complications [41].
At our center, FQP has been temporarily discontinued in the stem cell unit but is still in place in patients undergoing intensive chemotherapy for acute leukemia. As a result, potentially resistant pathogens, including P. aeruginosa, may be already selected prior to stem cell transplantation.
As previously shown, FQP, prior antibiotic therapy with either piperacillin/tazobactam or a Pseudomonas-carbapenem, and hematological disease are risk factors for BSI with MDR P. aeruginosa.
Antibiotic stewardship in hematology may therefore contribute to reducing infections caused by multi-resistant pathogens and the maintenance of a protective microbiota, thereby improving patient outcomes [42].
As a consequence of our study, we would like to strengthen antibiotic stewardship efforts on hematology wards. In the light of the observed increase in mortality associated with FQR, the use of FQP in patients with acute leukemia under intensive chemotherapy should be reconsidered.



留言 (0)