To the best of our knowledge, this study is the first one to analyse treatment failure of patients with VO and an underlying malignancy. We present a comprehensive analysis of VO patients with an underlying malignancy and VO patients with CKD compared to VO patients without comorbidities, focusing on clinical characteristics, causing pathogens, outcome, and risk factors for treatment failure within the first year after diagnosis of VO. Our most important and significant results were the following: (i) Every fourth VO patient (26%) with a malignancy suffered from treatment failure within the first year after diagnosis of VO. (ii) VO patients with CKD showed a strikingly high treatment failure of 45%. (iii) The distribution of VO-causing pathogens in patients with a malignancy differed explicitly from the other groups. CoNS (27.3%) were the most common causative bacteria in the ONCO group, followed by S.aureus (22.7%) and gram-negative species (15.9%). (iiii) S.aureus as underlying bacteria in VO patients with a malignancy, the presence of bacteraemia in VO patients with CKD and the presence of IE in VO patients without comorbidities could be identified as independent risk factors for treatment failure, respectively.
Clinical characteristics of VO patients in our cohort did not differ from VO patients in other studies [9]. Since comorbidities are known to be associated with high mortality in patients with VO [12, 16], the high CCI score of the ONCO patients (score ≥ 5 in 68% of cases) and CKD patients (score ≥ 5 in 75% of cases) in our cohort might be one factor contributing to the high treatment failure. In the ONCO group, diabetes, heart failure and COPD were the most common comorbidities but each occurred in less than 20% of patients. In contrast, almost half of the CKD patients had a secondary diagnosis of diabetes and heart failure. This can most likely be explained by the fact that CKD and heart failure are common long-term consequences of diabetes. The high co-occurrence of diabetes and heart failure in patients with CKD may have significantly contributed to the high treatment failure rate in this population. Diabetes increases the risk of mortality and leads to poor prognostic outcomes, while congestive heart failure is associated with a significantly higher mortality rate. [19, 21]. VO patients of the CONTROL group were mainly categorized as mildly comorbid (≤ 2) by the CCI score. However, 42% of CONTROL patients were categorized as moderately comorbid which can be explained by age as a contributing factor. In the CCI score, people aged above 70 years are already classified as moderately comorbid.
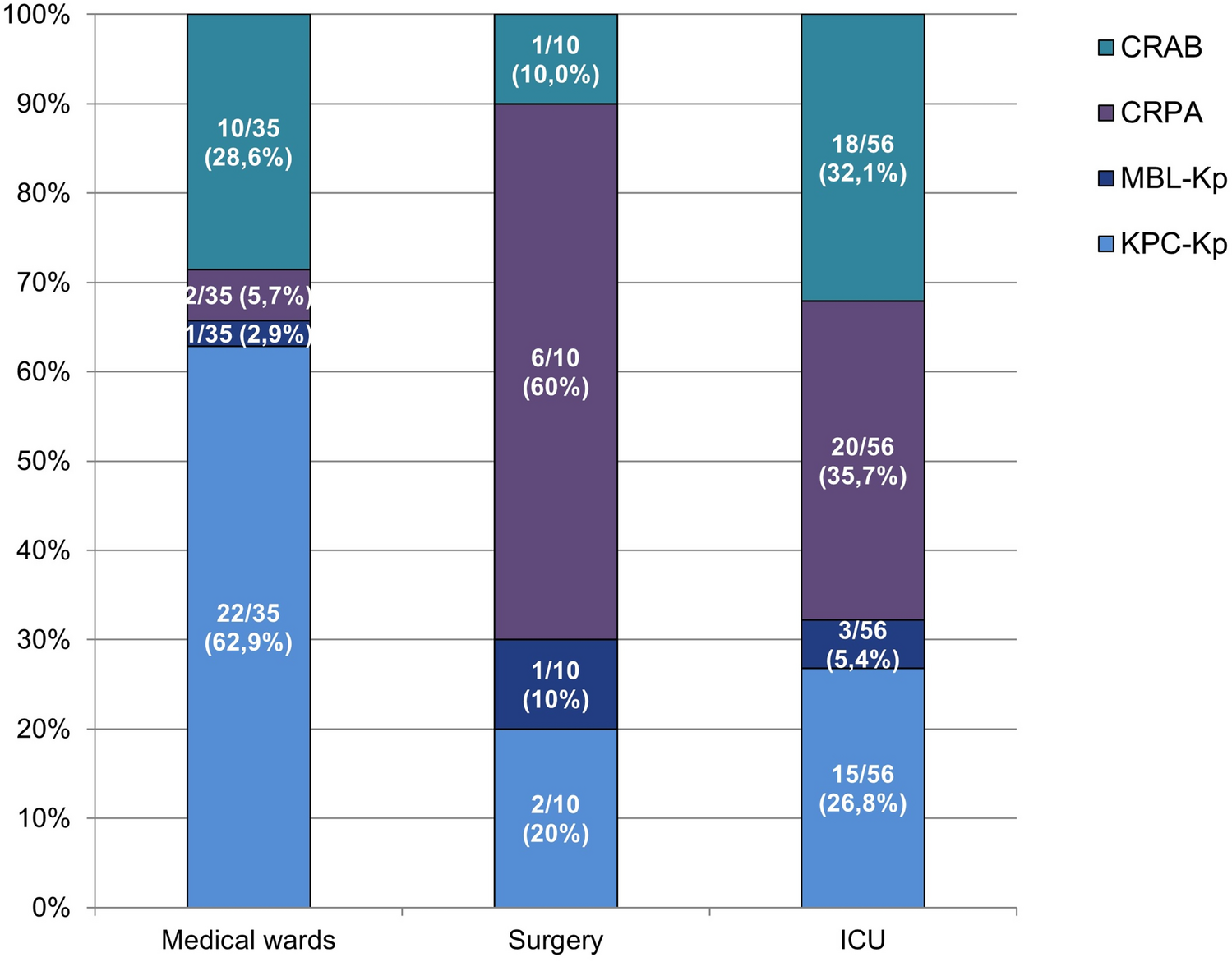
S.aureus is known to be the most common pathogen causing VO in Europe [9, 22,23,24,25,26]. In addition, several studies have found that the prevalence of S.aureus is particularly high in CKD patients [20, 27,28,29,30,31]. This is in line with our findings. In our study, S.aureus was the most frequent causing pathogen of VO in the CKD and CONTROL group. S.aureus could be identified in more than half of the CKD patients (56.7%) as well as in 42% of the CONTROL group. Only CoNS were accounting for another relevant amount of approximately 20% of VO in the CKD as well as the CONTROL group. Apart from this, every other bacterial species was found in less than 10% of CKD and CONTROL patients.
In contrast to the CKD and CONTROL group, VO ONCO patients in our study showed a broad distribution of VO-causing pathogens: CoNS, S.aureus, Streptococcus species and gram-negative species each accounted for at least 10% of vertebral infections in the ONCO group. S.aureus was responsible for only 23% of VO in the ONCO group, while CoNS were the most frequently detected specimen in ONCO patients, accounting for 27% of cases. Candida species as underlying pathogens could exclusively be found in the ONCO group. The wide range of causative bacterial species in the patients with an underlying malignancy might be a result of immunosuppression and different infectious pathways. These include, in particular, endogenous infections, e.g. due to mucositis or enterocolitis, nosocomial acquired infections, especially venous catheter-associated infections, as well as community acquired infections with haematogenous spread. CoNS are part of the skin flora and frequently occur as causative pathogens following surgical procedures [32]. In addition, CoNS are frequent pathogens of vascular catheter-associated bacteraemia. Accordingly, CoNS were the most frequently found bacterial species in patients with a malignancy and a central venous catheter-related infection [33]. This is consistent with the high prevalence of CoNS in our ONCO group. ONCO patients are particularly at risk of infections caused by CoNS due to mucositis and the frequent use of central venous catheters for chemotherapy or in case of parenteral nutrition.
Candida species and gram-negative bacteria are part of the intestinal flora and can lead to bloodstream infections in oncological patients with mucositis or enterocolitis. In our study, gram-negative species were detected twice as often in the ONCO group as in the CKD and CONTROL group. The high incidence of gram-negative species in ONCO patients can be supported by the results of two retrospective studies from 2015 [34] as well as 2020 [29], which could find a significant association of the presence of gram-negative bacteria in VO patients with a malignancy. Overall, patients with malignancies show a higher rate of infections caused by gram-negative bacteria than by gram-positive bacteria [35]. With regard to vertebral infections, we were able to show that gram-positive pathogens were responsible for two thirds of VO in ONCO patients. Other risk factors for VO caused by Candida spp. are immunosuppression and the use of broad-spectrum antibiotics [36, 37]. Both risk factors are common in oncological patients. VO caused by Candida species is rare but accounts for an overall mortality of 15% [36].
To date, there are no studies which explicitly deal with VO patients with an underlying oncological disease that could be compared with our results. It is known from a large retrospective Japanese study including 7118 VO patients that malignant diseases are associated with a higher rate of in-hospital mortality (OR: 2.68; 95% CI 2.10–3.42) [16]. In our cohort, the risk of treatment failure in oncological patients was five times higher when S.aureus was detected as the causative pathogen (OR: 4.600; 95% CI 1.749–12.100; P = 0.002) although S.aureus was less common in ONCO VO patients than in the other groups. The presence of S.aureus bloodstream infection (SAB) is known to be associated with high mortality in VO patients in general as well as in oncological patients [12, 23, 38]. Regarding oncological patients, in a 14-year nationwide study in Denmark on SAB in haematological patients, a mortality rate of 44% was demonstrated [39]. A similar mortality rate of 41.2% (49/119) could be found in non-neutropenic cancer patients with SAB in a study from 2012 by Kang et al. [40]. These study results support our finding that S.aureus is an independent risk factor for treatment failure in oncological patients.
In the subgroup analysis of oncological VO patients, the entity of the malignancy did not show any significant association with treatment failure. An active malignancy was only significantly associated with treatment failure in the univariable analysis. This might be due to the small number of cases compared to the overall collective. Though we could not show that an active malignancy is an independent risk factor for treatment failure, we advise to reinvestigate this question in further studies.
Almost half of the CKD patients in our cohort died within one year after VO diagnosis which is highly concerning. The most commonly reported 1-year mortality rate in VO patients with CKD in literature is lower than in our cohort and accounts for approximately 20–25% of patients. In 2024, Ratiu et al. performed a comprehensive literature review and identified only 18 relevant studies on VO in haemodialysis (HD) patients which reveals the limited experience and sparse data available on VO patients undergoing HD [41]. In a systematic review from 2019 about VO with end-stage renal disease including 30 articles with 212 patients in total, the reported overall mortality was 24.1% [20]. In a study from 2017 by Lu et al. including 102 VO patients undergoing HD, 1-year mortality was 21.6% but there was an additional 20% of patients who suffered from recurrence within one year [27]. This result is comparable to the high treatment failure in our CKD group. However, in our cohort, recurrence did not occur in any of the CKD patients. Instead, every CKD patient with VO who suffered from treatment failure died. Bacteraemia increased the risk of treatment failure threefold in the CKD group regardless of the pathogen (OR: 3.400; 95% CI 1.254–9.216; P = 0.016). Bacteraemia is expected to cause kidney injury due to inflammation and ischemia which, as a result, leads to further decreased kidney function in CKD patients and therefore to more complications [21]. This highlights the importance of blood culture-samples, both as diagnostic tool and as prognostic factor.
Strengths
To the best of our knowledge, this is the first study analysing VO patients with an underlying malignancy. As we compare different comorbidities, namely oncological patients versus CKD patients versus otherwise healthy patients, our study provides comprehensive information on a broad range of patients at risk of VO and their risk factors for treatment failure. Another strength is the 1-year-follow-up study design. By focusing not only on mortality but on treatment failure within one year after diagnosis of VO, our results add important information about the course of disease.
Limitations
Because of the monocentric study design, our results might not be fully representative. Therefore, we advise to perform an additional prospective, multicentre cohort study to verify our findings. In addition, our data did not provide sufficient information about whether the events of death were clearly related to the infection itself, to the underlying disease or to other causes.



留言 (0)