Respiratory support strategies in neonatal transport in the UK and Ireland
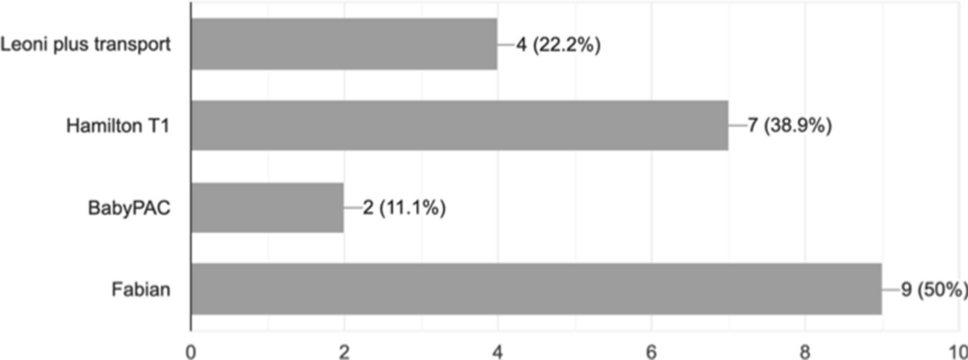
We have demonstrated that ventilators used in neonatal transport differ from those used in NICUs. The mechanism of action of the ‘Hamilton T1’ ventilator is via turbine air extraction which is not commonly used in NICU ventilators. Furthermore, the ‘Leoni plus’ has an alternative internal configuration when compared to the ‘Leoni’ used in NICU; the alternative internal configurations reduce shock effects. While the ‘Fabian’ ventilator used in transport is the same as in NICUs, it does not have certification for use in transport. It has not been reported whether the Fabian ventilator requires internal configuration changes similar to Leoni ventilators to ensure performance during transport. Bench testing has demonstrated that different neonatal ventilators deliver different volumes despite identical ventilator settings, particularly in premature models [7]. Differences in ventilator performance may then result in delays to stabilisation which has been highlighted as a quality metric to assess performance of a specialised neonatal transport programme [8].
VTV was the most commonly used invasive mechanical strategy during neonatal transport. It has been shown to reduce the occurrence of excessive tidal volumes (VTe > 8 ml/kg) and was associated with lower mean VTe compared to pressure-controlled ventilation (4.8 versus 6.0 ml/kg; p = 0.0011) during neonatal transport [9]. Excessive volumes in the delivery suite have been associated with intraventricular haemorrhage [10]. Whether they have a similar adverse effect during early transfer of prematurely born infants merits investigation. A retrospective observational study demonstrated that during both HFOV and HFOV-VG, ventilator parameters are maintained close to their targets during transport [11] whether this improves outcomes merits investigation.
In an attempt to reduce the incidence of bronchopulmonary dysplasia (BPD), there has been an increased focus on using non-invasive ventilation, and this has been reflected by changes in neonatal transport respiratory support strategies over the last two decades. In this survey, all transport teams were using non-invasive ventilation with the most common being HHFNC. Randomised trials of HHFNC versus CPAP amongst infants on neonatal units, however, have shown that HHFNC is less successful than CPAP in supporting premature infants [12]. Furthermore, if CPAP fails, there is a higher rate of pneumothorax, longer durations of respiratory support and hospital stay as well as a higher rate of BPD and death [13]. Thus, non-invasive ventilatory strategies during neonatal transport should be evaluated and compared.
There is a paucity of data on the use of capnometry during neonatal transport. Our survey demonstrated that the majority of transfer teams were using continuous CO2 monitoring. A UK neonatal transport audit reported variation in rates of hypocapnia (0–10.3%) and hypercapnia (0–9.4%) [5]. Using international transport databases and the UK Neonatal Transport Group data submissions, local and national rates of ventilation and normocapnia were tracked. It was demonstrated that volume-guided ventilation and transcutaneous CO2 monitoring had a positive influence on the maintenance of normocapnia during transfer [14]. Whether this influences longer term outcomes needs to be determined.
Two groups reported the use of CLAC using Fabian ventilators. An evaluation of quality metrics to assess performance of neonatal transport programmes included desaturations/cyanosis episodes as one of four physiological parameters to be used [8]. CLAC in the NICU has shown to reduce the incidence and duration of hypoxemic episodes in ventilated infants both those born prematurely and at term. Its use during transport of infants requiring escalation of care thus might improve outcomes.
We designed the survey with a limited number of questions, as we have previously found this resulted in a better response rate. We have, however, subsequently contacted the teams regarding their heating and humidification practices and the longest distances over which they transported infants and included this information. We did not ask the teams if they used particular strategies for particular conditions, as there is no evidence that a particular strategy would benefit infants with certain conditions during transport.




留言 (0)