
記住我

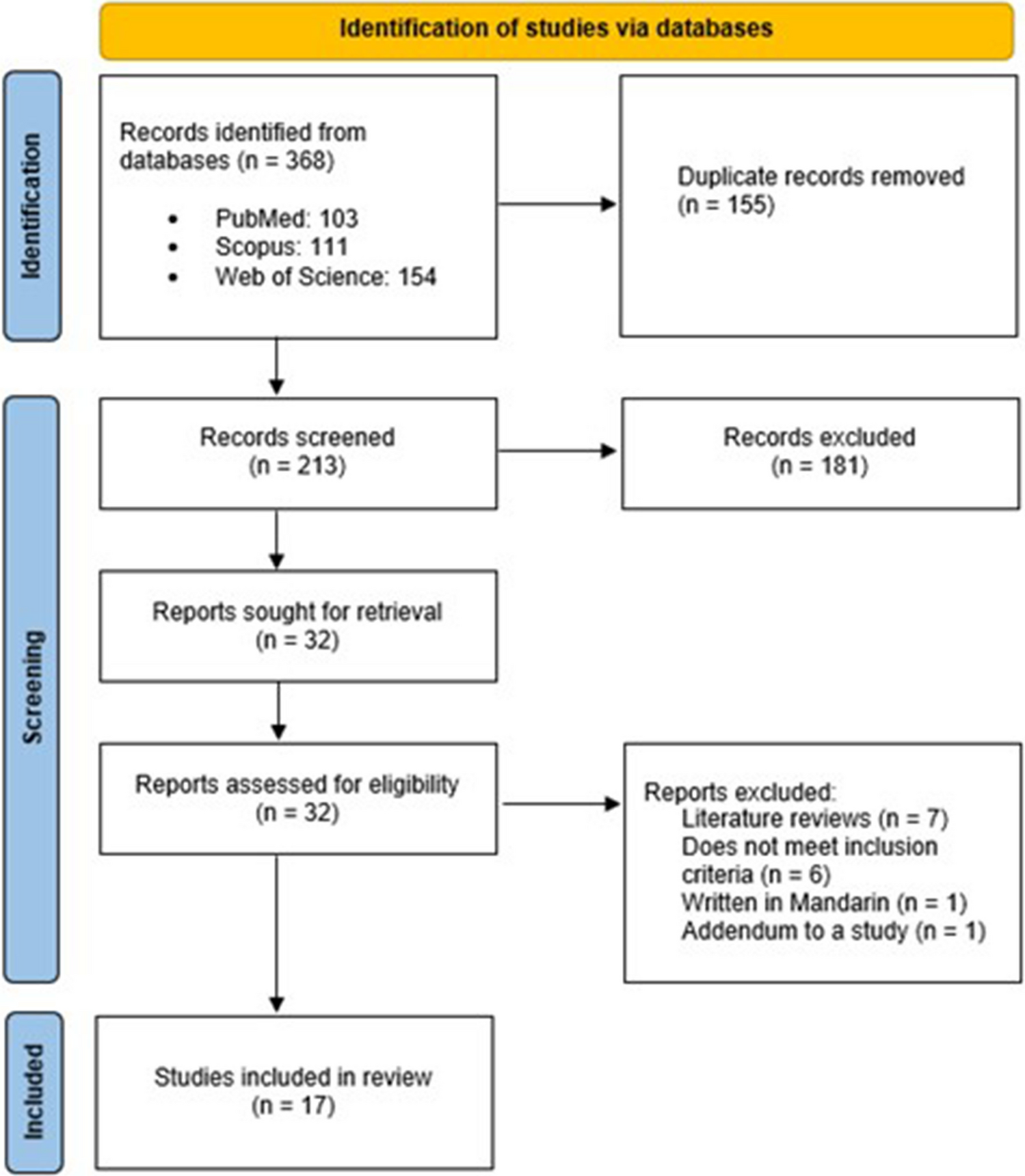


A total of 1618 articles were identified through the search strategy as depicted in Fig. 1. After removing the duplicates and screened for title and abstracts, 35 full text articles were screened for eligibility. The excluded articles did not meet the eligibility criteria, such as did not meet the study objectives, study participants of infants with congenital diseases or jaundice, or the paper was not peer-reviewed. The final number of articles selected for this scoping review was 25.
Among the 25 articles included, there were 16 review articles, consisting of 12 narrative reviews, one scoping review, and three systematic reviews. There were six experimental studies retrieved, of which one was a nested intervention study, and four randomized controlled trials. Additionally, there were three observational studies retrieved, with two cross-sectional studies and one with longitudinal design. The studies were conducted in different regions, namely Europe (n = 11), North America (n = 7), Asia (n = 6), and South America (n = 1).
Observational studiesIn terms of observational studies as seen in Table 2, a cross-sectional study with 22 infants was conducted to determine the association of light exposure and circadian rest-wake activity [17]. Light exposure and rest-wake activity were determined using a light-activity actigraphic monitor and a sleep-activity record. Another cohort study involved 72 healthy 8-month-old infants which assessed the sleep architecture during different seasons of birth (spring, summer, autumn, and winter) [18]. Infants were divided into four subgroups representing the four birth seasons with different levels of light exposure and underwent ambulatory overnight polysomnography. Another recent cross-sectional study was conducted among 43 infants to determine the role of light exposure and co-sleeping with sleep consolidation into nighttime [19]. Infant sleep parameters were recorded using actigraphy for four consecutive days, while light stimulation and co-sleeping behavior data was obtained from a sleep events diary and questionnaire respectively.
Table 2 Observational studies (n = 3)Experimental studiesExperimental studies were focused among preterm infants in hospital environment, whereby the common aim was to determine the outcomes of preterm infants in different light environments [Table 3]. Guyer et al. (2015) had an experimental group with 34 preterm infants, while 14 term infants were selected as control [12]. Another randomized interventional study compared 38 preterm infants in NICU grouped into light–dark cycle group and continuous light group [20]. Intervention groups from both studies were exposed to cycled lighting by allowing light exposure from 7 a.m. to 7 p.m. and off during other timing. Lighting to imitate “dark” hours were done by installation of bed curtains, usage of quilts on incubators, or using a specially designed acrylic helmet. Assessment of circadian rhythm was found to be done using actigraphy recording or salivary melatonin rhythm. On the other hand, a randomized controlled trial had a group of 42 preterm infants randomly assigned to either experimental group with red LED light, or control group with white LED light exposure at night, both groups having approximately the same level of daytime lighting exposure [13]. Actigraphy data was obtained to assess the activity during daytime and nighttime. The study conducted by Watanabe et al. reported infants in the experimental group were placed under a light filter which cuts the wavelength that could be detected by melanopsin and rhodopsin in the eye, while the control group infants were placed in normal clear covers. The light filter mimics an artificial night in a continuous bright light environment in the NICU, which provides a light–dark cycle environment to the infant [21]. Similarly, using an incubator cover, Varvara and colleagues reported that there was increased duration of deep sleep as the intensity of light at night mimics near darkness to consolidate sleeping patterns among preterm infants [22]. On the other hand, Valizadeh et al. conducted a randomized controlled trial which both groups were placed into incubators with thick cover, while the intervention group had face covers to reduce light exposure [23]. It was observed that sleep duration was significantly longer among the intervention group, while the control group had decreased sleep periods instead.
Table 3 Experimental/intervention studies (n = 6)Review studiesThe findings of the review articles from Table 4 were explored in a few themes, such as the periods of infant circadian rhythm development, consequences of infant circadian rhythm disruption, cycled lighting vs continuous lighting, and other recommended lighting conditions.
Table 4 Review studies (n = 16)The phases of infant circadian rhythm developmentThe infant circadian rhythm development involving light exposure occurs in four phases. Firstly, the main oscillator of the circadian rhythm, the SCN, starts developing during the fetal phase; however, it is only coordinated during the postnatal period [8]. The entrainment of infant circadian rhythm is guided via environmental cues and breastmilk consumption, which was influenced by content of melatonin and cortisol during the postnatal period [24]. Next, the infant cortisol rhythm responsible for wakefulness develops as early as 8 weeks, followed by melatonin rhythm establishment at approximately 9 weeks for sleep onset [2]. The maturation of visual pathways is the last phase which occurs around 39 to 40 weeks after birth with proper exposure of rhythmic ambient lights to entrain the circadian rhythm [25]. During the neonatal period, the VIP-expressing neurons of the SCN continues to develop and reaches full maturation by the first 2 years of life [24]. Hence, the entrainment of infant circadian rhythm occurs in separate stages before the full maturation of the SCN, indicating the need for optimum environmental cues such as avoiding artificial light at night and maternal breastfeeding, to ensure the development of SCN pathway.
On the other hand, preterm infants had different phases in circadian rhythm development. From Escobar et al. (2021), the circadian rhythm of preterm infants is not apparent until 6 weeks after birth [9]. Preterm infants were also found to have prematurely lost the circadian connection from the pregnant mother, and their circadian rhythm was replaced with environmental cues following the light–dark cycle. This can be noted from the distinct sleep–wake rhythm development of preterm infants when placed under cycled light compared to term infants who were placed under the same conditions, indicating the role of external time cues may mask the influence of the maternal rhythm [24].
Difference in seasonal effects will also determine the circadian rhythm development due to the different photoperiods. Shorter photoperiods during autumn and winter were related to more “early-morning” types born, and more “night owls” born during spring and summer with longer photoperiods, and this effect is most prominent among population from higher latitudes where the variation of photoperiod is greatest [26]. Seasonal variation of birth time had an impact on infant’s sleep at 8 months, notably infants born in spring had less slow wave sleep (N3) and longer stage two non-rapid eye movement (N2) sleep compared to those born in autumn [18]. This finding was consistent with another large cohort study with 1302 pairs of mother-infant dyads, reporting that although infant sleep patterns are similar to their mothers, their nighttime sleep duration was longer during spring compared to autumn [27].
Consequences of infant circadian rhythm disruptionThe infant’s lighting environment can disrupt the circadian rhythm development by affecting their sleep–wake cycle. The disruption of circadian rhythm during early life implicates the etiology of mood disorders such as schizophrenia [28]. Circadian dysfunction at the developmental stage of life was also associated with brain disorders such as autism, depression, and Parkinson’s disease [29].
Cycled lighting vs continuous lightingCycled lighting was deployed to simulate the daytime and nighttime environment, and was reported to influence hormonal production which is essential in the healing processes [30]. It has been a favorable method to entrain the infant circadian rhythm, as observed from reduced fussiness and improved sleep [11]. A regulated behavioral state after birth can be assessed by reduced daytime crying patterns and consolidated sleep [31]. From the study, the cycled light group showed a day and night period of 23.99 ± 0.04 h, while the dim light group was longer than the 24-h period with 24.77 ± 0.3 h as measured using an actigraphy watch. This shows that cycled lighting can entrain the sleep–wake rhythm to adapt to the 24-h light dark cycle. Studies also found that infant circadian rhythm was entrained with a low intensity (200 lx) cycled light environment rather than constant dim light [24].
Among preterm infants, sleep–wake cycle synchronized with the 24-h light dark cycle was found to shorten the period of hospitalization and promoted the adaptive responses such as heart rate, food responsiveness, and body weight when exposed to more than 2 weeks of cycled lighting [24, 26, 32, 33]. Light reduction was also shown to improve infant stability, including their respiratory rate and heart rate [34]. It was also reported that cycled-lighting was beneficial and showed no detrimental effects compared to continuous lighting or darkness [35]. Regardless, the lighting conditions should be personalized according to the infants condition, healthcare providers’ visibility to conduct nursing care, and tools used for lighting protection [36].
Observational studies have shown that cycled lighting plays an important role in establishing the infant circadian rhythm, particularly in aligning the sleep–wake schedule according to the 24-h light dark cycle. Cycled lighting was found to contribute to longer nighttime sleep duration between midnight and 6 a.m. among preterm infants compared to term infants, while dim light exposure resulted in less active preterm infants [12]. It also promoted rapid weight gain and significantly decreased the duration of hospital stay for preterm infants, as well as reducing nosocomial infection [20]. When investigating the role of different colors of LED light on preterm infants’ rest-wake activity patterns, there were no significant differences between control (white LED light) and experimental groups (red LED light) [13]. Preterm infants were not able to detect the red LED light with a wavelength of > 675 nm as the retinal photoreceptors were premature. On the other hand, the white LED light consists of a wider range of wavelengths which the preterm infant was able to receive. However, the brief white light exposure was overwhelmed by the effects of cycled lighting. Hence, the development of infant circadian rhythm mainly depends on the light exposure according to the 24-h light dark cycle instead of the color of light source. A summary of cycled lighting timing, intensity, and its outcomes from the reported studies was depicted in Fig. 2.
Fig. 2
Timing, intensity, and outcomes of cycled lighting exposure. This figure is based on the findings of this review which excludes natural light exposure
Other recommended lighting conditionsWhen the lux levels remained constant at 249 ± 11 lx, melatonin level was not stimulated and remained low, while cycled lighting of 249 ± 11 lx during the day and 27 ± 0.8 lx at night exhibited a daily rhythmicity of salivary melatonin among preterm infants [9], while Morag et al. suggested that cycled lighting conditions can be defined as less than 20 lx for 12 h at night, greater than 200 lx for 12 h during the day [33]. Rodriguez et al. stated that cycled light with 100 to 200 lx during the day and artificial light lower than 50 lx should be implemented in NICU settings [34]. There were also studies reported that standard levels of hospital lighting was 400 to 1000 lx, while the recommended levels should be 10 to 600 lx [26, 37].
There is a need to balance the preservation of nighttime darkness with lighting conditions to perform medical procedures safely in the NICU as even a short period of 5 min of bright light exposure can delay the melatonin phase by 3 h [26]. Hence, protective accessories to avoid bright light exposure such as infant goggles or helmets, and installing a light filter in incubators could be implemented to retain the dark condition [21, 26]. Other strategies such as health promotion programs to increase awareness of the importance of sleep and circadian health should be executed, as well as providing sufficient human resource and technical support [38]. From observational studies, results showed that duration of light exposure with intensity of more than 500 lx was a significant predictor of infant circadian rhythm development measured by greater amplitudes in acrophases of rest-wake activity (β = 0.50, p = 0.01), indicating stronger circadian activity [17]. Recent studies looking into lighting environments in home settings have reported that more daytime light exposure was associated with improve daytime wakefulness of infants and improves sleep efficiency at night, indicating less nighttime waking and prolonged night sleep for the infant [39].
留言 (0)