
記住我



Between 2010 and 2014, 130 patients with synchronous or metachronous brain metastases from gastrointestinal tumours were included in the study, either with CRC (105; 80.8%) or EGC (25; 19.2%) (Table 1). Among them, 84 (64.4%) were women, and the median age was 66.0 (28.0–92.0). A fraction of patients (21/130;16.2%) did not receive any chemotherapy before brain metastases diagnosis. Unfortunately, lines of chemotherapy were not completed enough to establish the number of lines of treatment before BM diagnosis. Most patients (125/130; 96.9%) presented with an adenocarcinoma, with well-differentiated tumours in 45 (37.5%) of cases. Patients had a T3 or T4 tumour status in 84 (87.5%) of cases, a T1 or T2 status in 12 (12.5%), and an unknown T status in 34 (26.2%) of cases; the N status was N0 in 26 patients (27.1%), N1 70 patients (72.9%), and unknown in 34 (26.2%) patients. At primary tumour diagnosis, 56 patients (48.7%) had a non-metastatic disease (M0), and 59 (51.3%) patients were metastatic (M1).
Table 1 Population and tumour characteristicsTable 2 Brain metastases diagnosis and treatmentTable 3 Multivariate analysis of significant variables in univariate analysis associated with overall survivalThe metastastic localizations (excluding BM) at BM diagnosis were mainly lung (81/130; 68.1%), liver (68/130; 57.1%), and lymph modes (38/130; 31.9%). The other sites were bone (17/130; 14.3%), peritoneum (11/130; 9.2%), and adrenal glands (8/130; 6.7%) (Appendix Table A1). The number of metastatic sites was one in 46 (38.7%) patients, two in 45 (37.8%) patients, and three or more in 28 (23.5%) patients. The median time for non-BM occurrence from cancer diagnosis was 3.3 months (range 0; 107.7). OS was respectively of 12.8, 4.2, and 0.1 months if 1,2 or 3 metastatic sites were involved (p = 0.147).
Brain metastases characteristics and managementNeurologic symptoms revealed BM in 120 patients (81.6%) (Table 2). BM diagnosis was confirmed on computed tomography (CTscan) in 100 (77.5%) patients and/or magnetic resonance imaging (MRI) in 80 (62.5%) patients and exceptionally by positron emission tomography (PET-CT) in 6 (4.7%) patients. Histological confirmation was obtained in 11 (8.5%) patients, primarily by surgery (9/130; 81.8%). BM were cerebral in 58.6% of patients, cerebellar in 12.1% and both locations in 29.3% of patients. BM sites were unique in 43.0% of patients, two in 21.1%, and three or more in 35.9%. Brain metastases were in the frontal lobe (29.7%), parietal lobe (23.9%), temporal lobe (21.7%), or occipital lobe (21.0%). They were most often unilateral (63%). Biomarkers were performed: CEA in 77 (81.1%) patients and/or CA19-9 in 17 (17.9%) patients. Markers were above the upper limit in 70 (73.7%) patients (Appendix Table A2).
Most patients (106/130; 84.1%) received a treatment upon BM diagnosis (Table 3). Symptomatic therapy for BM symptoms was given to 106 (84.1%) of patients: corticoids in 100% of cases and Mannitol in 18.4%. A curative treatment was intended in 101 patients (77.7%), either surgery (24/130; 18.9%), among which 22 (95.7%) resections, or radiotherapy (33/130; 25.8%). Most patients treated with radiotherapy received whole-encephalic radiotherapy (70/130; 79.5%). The median dose was 30 Gy (range 8–30). Among treated patients, 39 had a brain progression during follow-up. Brain-progression free survival was 19.6 months, (95CI:10.6–26.2) in CRC patients and non-achieved in EG patients (p = 0.203).
We further explored the impact of BM location on treatment access comparing patients with cerebral metastases with no cerebellar metastasis (N = 73) versus patients with cerebellar metastases (N = 51) (Appendix Table A3, N = 124 patients as BM location was missing for 6 patients). To increase power, all patients with a cerebellar lesion were included in the latter group, regardless of its association with (N = 34) or without (N = 17) a cerebral lesion,. The number of brain lesions was significantly higher in patients with cerebellar metastases group (p = 0.0002), with a high number of patients with 5 brain lesions or more (2.8% vs. 29.4%). Non-classical BM locations were also more frequent in those patients (11.3% vs. 56.9%, p = 0.0001). The neurological symptoms leading to diagnosis (82.2% vs. 84.3%, p = 0.757) were not increased in patients with cerebellar metastases. Accordingly, there was no difference in administration of symptomatic treatment (81.4% vs. 88.2%, p = 0.309). There was a non-significant trend of a better WHO performance status (PS 0/1 = 51.5% vs. 40.0% and PS 2–4 = 48.5% vs. 60.0%) in patients with cerebellar metastases. The less frequent BM surgical treatment performed in patients with cerebellar metastases (24.3% vs. 11.8%) was not significant either and there was no difference in radiotherapy.
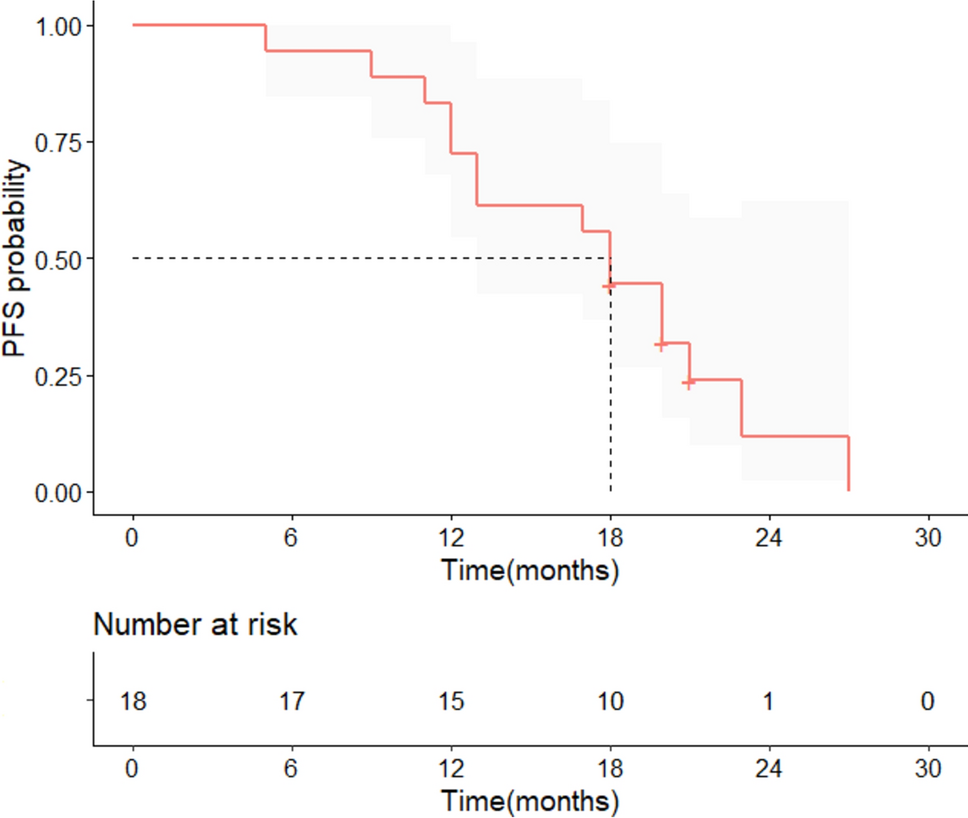
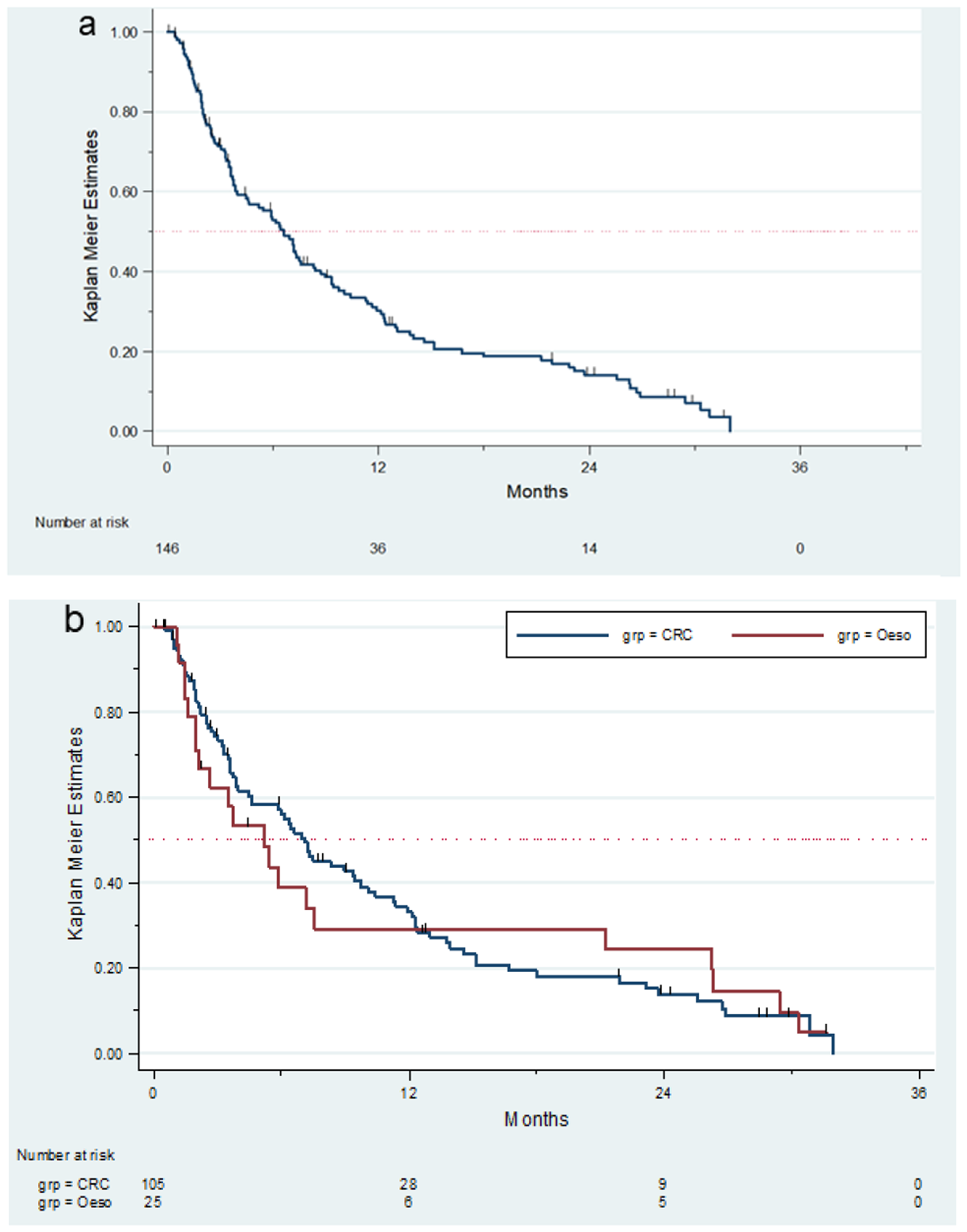
Survival and prognostic factorsFig. 1
Overall Survival. a. Total cohort b. patients with colorectal cancer (CRC) and oesogastric cancer (Oeso)
The median overall survival was 6.6 months (95CI:4.5–8.3) (Fig. 1A.) in the whole population, 7.1 months (95CI:4.47–9.72) in CRC patients, and 5.2 months (95CI:1.97–7.55) in patients with EGC primary tumour (Fig. 1B.). The survival rate at six months, one, and two years were, respectively, 53% (95CI:44–61), 30% (95CI:22–38) and 13.6% (95CI: 08–21; 2 patients).
In univariate analysis (Appendix Table A4 and A5), the Recursive Partitioning Analysis (RPA) prognostic classification, taking into account the patient’s age (< 65 years), the general status (Karnofsky > 70), and the absence of non-brain metastases, showed a non-significant trend for patients with higher scores, meaning worse condition. In multivariate analysis (Table 3), several prognostic factors were identified. BM location (p = 0.022; 95CI:1.09–3.13), BM surgery (p = 0.013; 95CI:0.29–0.90), WHO Performance status (p = 0.005; 95CI:1.19–2.78), and the BM number (p = 0.021; 95CI:0.30–0.90) were significantly correlated with OS. OS was significantly longer in patients with cerebral metastases (8.7 months, 95CI: 5.9–12.3) compared with patients with cerebellar metastases (4.6 months, 95CI:1.3–7.2) or both (3.7 months, 95CI:2.4–7.5). Patients who underwent BM surgery had a longer OS, 12.1 months (95CI:7.2–18.0) versus 4.6 months (95CI:3.6–7.2) in patients who did not undergo surgery for brain metastasis. A WHO performance status of 0 or 1 was associated with longer overall survival (8.4 months, 95CI:6.6–11.3) than a performance status of 2 (3.3 months, 95CI:2.4–5.9).
Factors associated with brain metastasis occurenceFig. 2
Brain Metastasis Free Survival curves of patients with colorectal cancer (CRC) and oesogastric cancer (Oeso). a. From disease diagnosis b. From diagnosis of metastatic disease
The median BM-free survival was 25.9 months (95CI:21.4–31.2) (Fig. 2A.) in the whole population and 27.6, 19.6, and 26.8 months in patients with 1, 2, and 3 or more metastatic sites, respectively (p = 0.188). In CRC patients, the BM-free survival was 30.8 months (95CI:25.1–36.9). There was no significant difference in the RAS status, which was assessable in 66 patients. In EGC patients, the BM-free survival was 7.8 months (95CI: 3.8–13.6).
The Stage 4 BM-free survival (Fig. 2B.) for the whole population was 14.7 months (95CI: 7.8–19.6). It was 18.6 months (95CI: 13.1–25.2) in CRC patients and 3.7 months (95CI: 0.03–7.8) in EGC patients (p = 0.001). In univariate analysis, the presence of lung metastases (p = 0.027 in CRC and p = 0.001 in EGC), a low number of the non-BM sites involved (p < 0.0001 in CRC and p = 0.004 in EGC), surgery of the primary tumour (p < 0.0001 in CRC, nonsignificant in EGC), and well-differentiated tumour (p = 0.016 in CRC, nonsignificant in EGC) were associated with longer stage 4 BM-free survival.
DiscussionMETACER prospectively confirmed a poor OS of 6.6 months for GI-cancer patients with BM. Patients with T3-T4 tumours (65.5%) and lung metastases (68.1%) were over-represented. Cerebral metastases, BM surgery, 0–1 WHO Performance status, and a unique BM were prognostic factors associated with prolonged OS. As cerebral CT scans are not performed systematically in the follow-up of GI-cancer patients, most of the patients had neurologic symptoms at BM diagnosis. Asymptomatic BM are reported as the majority of BM (79%) diagnosed upon screening for clinical trials in metastatic CRC [5].
As for BM management, 22.3% of METACER patients were not considered for treatment, likely due to poor condition. Among those achieving treatment, less than 20% had access to surgery, which, when performed, resulted in R0 resection in more than 95% of cases. Other patients received whole-brain radiotherapy (79.5%) and/or stereotactic radiotherapy (26.5%). The Vienna Registry showed that stereotactic radio-surgery (SRS) had already spread by 2010 [2] and it was reported in a series of patients with BM from CRC in 2011 [13]. However, its use in an adjuvant setting was validated in 2017 [26] which may account for the low rate of SRS in METACER. SRS delivers a higher dose on lesions and allows repeated treatment while maintaining a good quality of life [27]. Nowadays, surgery is frequently combined with SRS, broadening the number of BM locations accessible to treatment. Systematic imaging in late metastatic GI-cancer settings might be considered to improve patient access to multimodal treatment and improve their survival. We expect that the DEMECIA study (NCT03694938), which includes all metastatic CRC patients within six months from the disease diagnosis and performs cerebral MRI yearly, will prospectively evaluate the impact of a systematic cerebral imaging and early BM treatment on quality of life in metastatic CRC patients.
In the European Association of Neuro-Oncology - European Society of Medical Oncology (EANO-ESMO) guidelines [11], prognostic factors are crucial in BM management decision-making. Most prognostic factors are determined based on retrospective studies. METACER confirms good performance status as a significant prognostic factor. As far as the number of BM is concerned, METACER shows that a unique location is of better prognosis, as suggested in a meta-analysis [28]. As the literature is contradictory about the impact of KRAS status in retrospective series [7, 22], KRAS status was collected in METACER and was not associated with OS in this prospective cohort. BM location appeared as an independent prognostic factor with shorter OS in case of cerebellar lesions. Patients with cerebellar metastases had a non-significant poor WHO performance status and less surgical treatment. Instead, they displayed significantly more numerous brain lesions, and non-classical brain locations, which parameters are therefore more prone to explain the poor prognosis of patients with cerebellar BM. In this study, non-classical brain locations meant non frontal nor parietal, temporal or occipital. Data collection did not allow further description but suggests these atypical locations may be overlapping not only with cerebellum but also brainstem and midline brain lesions, which are hardly accessible to surgical treatment. In contrast to another study in breast cancer [29], no increase in neurological symptoms were observed in patients with cerebellar metastases. However, this BM location remained an independent prognostic factor in the multivariate model, which included also WHO PS and the number of BM locations. This result suggests that the over-representation of non-classical BM locations in patients with cerebellar metastases may explain their poor prognosis. As these are subgroups analyses, these data may be underpowered, therefore, must be interpreted with caution.
This study has several limits. First, the molecular profile of the GI primary tumour was incompletely collected. Especially, HER2 status was not collected whereas it now appears as enriched in EGC cancer patients with BM in the available retrospective studies [10]. This limit is linked to the date this cohort was designed and conducted. However, the prognosis of GI tumours with brain metastases has not evolved a lot since 2010 and remains lower than 10 months in the literature [1, 2, 9, 10]. This was carefully examined in the Vienna Brain Metastasis Registry [3], in which no significant difference in OS was noted between 1986 and 1999 / 2000/2009 / 2010–2020 with a median OS of four, five, and six months, respectively (p = 0.091). Furthermore, CRC data in METACER align with data collected in 351 patients with colon cancer BM from the Vienna Brain Metastasis Registry [3]. Then, patients were enrolled upon BM diagnosis, making the data collection between primary tumour and BM diagnosis primarily retrospective. Therefore, predictive factors of BM in this study remain exploratory. This may account for the result in a univariate analysis showing that lung metastases correlate with longer stage 4-BM free survival in both CRC and EGC, whereas lung metastases were reported as enriched in patients with BM from GI cancers [20, 23]. Its prospective nature conveys METACER’s main strength, as prospective data are very scarce in GI cancer patients with BM.
留言 (0)