
記住我


A total of 257 admissions (n = 248 participants) were included in the analysis. Nine participants were followed up during two separate admissions. Data sampling ended prematurely for 115 admissions due to discharge to another care setting. Of the remaining participants (n = 142), 62 died without and 80 participants with palliative sedation. During the palliative sedation period, discomfort levels were monitored for 78 participants; two of whom were lost to follow-up.
Most participants (n = 36, 46%) were admitted to a hospice setting, one third (n = 23, 29%) to hospital wards, and the remaining 24% (n = 19) to PCUs. Regarding sex, the number of male (n = 36, 46%) and female (n = 42, 54%) participants was almost equal, and the mean age of the participants was 69 years (SD 12.3). Table 1 shows all baseline characteristics.
Table 1 Baseline characteristics (PALSED study), total and per settingTable 2 shows that palliative sedation was initiated mostly for two symptoms (n = 31, 40%) or for a cluster of three or more symptoms (n = 32, 41%). The three most reported primary indications for starting were dyspnea (n = 17, 22%), delirium (n = 14, 18%), and exhaustion (n = 13, 17%). Predominantly, palliative sedation was started directly as continuous sedation (n = 73, 94%). In five participants, sedation was intermittently administered, and this modality was used until death in three participants and changed to continuous sedation for two participants. In the total sample, palliative sedation had a median duration of 38 h [IQR 16–88]. In two patients, the dose of medication was reduced until cessation, and the patients died comfortably without the use of sedative medication.
Table 2 Palliative sedation characteristics (PALSED study), total and per settingMidazolam was the first-choice sedative medication for all participants. Midazolam was started and continued at low (< 2 mg/h), moderate (2–5 mg/h), and high dosages (> 5 mg/h) in 31, 25, and 4 of patients, respectively. Adjustments were made to the administered midazolam dosages in 18 participants (23%). In 64% of the sample (n = 50), only midazolam was used, with a total median dosage of 2.0 mg/h (IQR 1.2–2.7). In two cases, midazolam was changed to another sedative, while another sedative medication was added to midazolam treatment in 26 participants. In those 28 participants, midazolam was administered with a median dosage of 3.0 mg/h (IQR 2.2–5.0).
For 78 participants who received palliative sedation, a total of 481 discomfort measurements were completed, with a range of 2 to 21 measurements per participant. In 7% (n = 32) of the measurements, there were missing data for the complete DS-DAT and RASS-PAL (n = 20) or for some missing DS-DAT item scores (n = 12). For two participants, the reasons for missing all measurements were loss to follow-up due to an acute start of palliative sedation and discharge to another hospital ward. From the pooled analysis of ten imputed datasets, we concluded that the outcomes shifted by less than 5% compared to the dataset with complete measurements only. Therefore, we used the database with complete measurements (n = 449 measurements) for reporting the results.
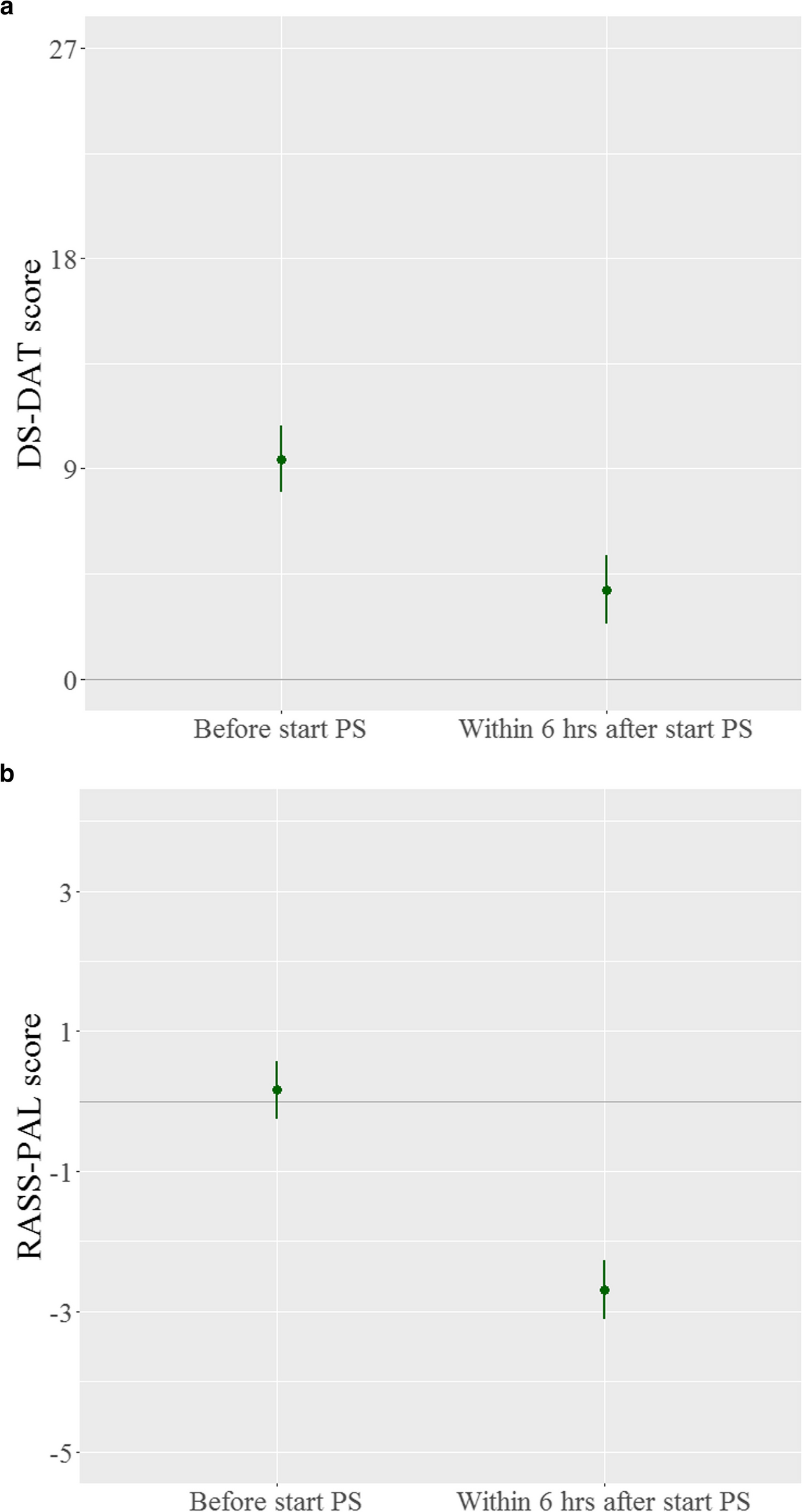
Comfort measurements after the start of palliative sedationIn the total sample, the mean discomfort score of 9.4 points (95% CI 8.0–10.9) at the start of sedation decreased by 5.6 points (95% CI 3.7–7.5) within 6 h after the start of sedation (Fig. 1a). When all discomfort measurements until the end of the sedation period were used to analyze the effect of palliative sedation, a decrease of 6.0 points (95% CI 4.8–7.1) was shown. Besides the initial effect of palliative sedation on discomfort, each hour increase in the sedation duration also resulted in a small decreasing effect by 0.02 points (95% CI 0.01–0.03) (Fig. 2). Figure 2 shows that in the multivariable analysis (red lines), no significant factors affecting discomfort levels at onset were found. Hospital ward patients had marginally greater mean scores on the DS-DAT (10.0, 95% CI 8.3–11.6), indicating greater discomfort before the start of sedation, while PCU participants seemed to have lower scores (8.6, 95% CI 6.9–10.3). However, the previously demonstrated decrease in discomfort levels remained unchanged after correction for age, sex, modality of sedation, and setting.
Fig. 1
a Effect of palliative sedation at discomfort levels (DS-DAT). PS, palliative sedation; DS-DAT, Discomfort Scale-Dementia Alzheimer Type. Measurement before start PS (n = 77): mean 9.4 points (95% CI 8.0; 10.9) Measurement within 6 h after start (n = 74): mean 3.8 points (95% CI 2.4; 5.3). b Effect of palliative sedation at sedation/agitation levels (RASS-PAL). PS, palliative sedation; RASS-PAL, Richmond Agitation-Sedation Scale modified for palliative care. Measurement before start PS (n = 77): mean 0.15 points (95% CI -0.27; 0.58); measurement within 6 h after start (n = 73): mean -2.69 points (95% CI -3.11; -2.27)
Fig. 2
Effects of palliative sedation (PS) and other variables at discomfort levels. PS, palliative sedation; PCU, palliative care unit; 95% CI, 95% confidence interval. Model 1. Repeated measurements model: mean discomfort before start: 9.4 (95% CI 8.3–10.5). Model 2. Multivariable model: repeated measurements model corrected for gender (ref = female), setting PCU and Hospice (ref = Hospital), Age (ref = mean age 69 years), Form: Intermittent sedation (ref = Continuous), mean discomfort before start: 10.0 (95% CI 8.3–11.6)
Sensitivity analysesFirst, the discomfort measurements (n = 421) of the participants (n = 75) who received continuous sedation at the time of measurement were evaluated. The results were comparable to those of the complete sample, which included intermittent sedation.
A second sensitivity analysis was performed to compare the outcomes of the midazolam group (n = 50) to those of the group in which also other sedative medications were used (n = 28). No significant differences in outcomes were found between the two groups. The data are not shown.
Levels of sedation and the correlation with discomfort levelsThe level of agitation/sedation was scored at the same time points as the discomfort measurements. Before the start of sedation, the mean RASS-PAL score was 0.15 points (95% CI -0.270.58), which decreased by 2.9 points (95% CI 2.6–3.3) after the start of palliative sedation, indicating deeper sedation (Fig. 1b).
A deeper sedation score, as measured with the RASS-PAL, correlated with a lower discomfort score (DS-DAT), with an r of 0.72 (95% CI 0.61–0.82). This relation was also revealed within a linear mixed model analysis. A decrease of one point in the RASS-PAL score, resulted in a decrease of 1.6 points (95% CI 1.4–1.8) at the DS-DAT.
As a sensitivity analysis, we also analyzed the range of measured discomfort score in participants with different depths of sedation. In participants with drowsy (RASS-PAL-1) to moderate sedation (RASS-PAL-3) measurements (n = 144, 32%), the DS-DAT scores ranged from no discomfort (n = 59, 41%) to minimal-moderate discomfort (score 1–7, n = 61, 42%) to high discomfort (score 8–27, n = 24, 17%). Most discomfort measurements in our sample (n = 200, 45%) were accompanied by a simultaneously measured deep sedation score. For those participants with RASS scores of -4 or -5, the DS-DAT ranged from no discomfort (n = 130, 65%) to minimal-moderate discomfort (score 1–7, n = 62, 31%) or high discomfort (score 8–18, n = 8, 4%).
DS-DAT scores in the sample of participants receiving palliative sedationIn the study sample, the internal consistency of the total DS-DAT had a Cronbach’s alpha of 0.83. All corrected item total correlations were > 0.35 (range 0.36–0.68), except for the “Noisy breathing” item, which had a lower correlation value (0.3). The Cronbach’s alpha increased to 0.85 when this item was deleted, while it decreased to less than 0.8 when the “Content facial expression,” “Relaxed body language,” or “Tense body language” items were deleted (see Table 3).
Table 3 Reliability statistics of the DS-DAT scale in the study samplea
留言 (0)