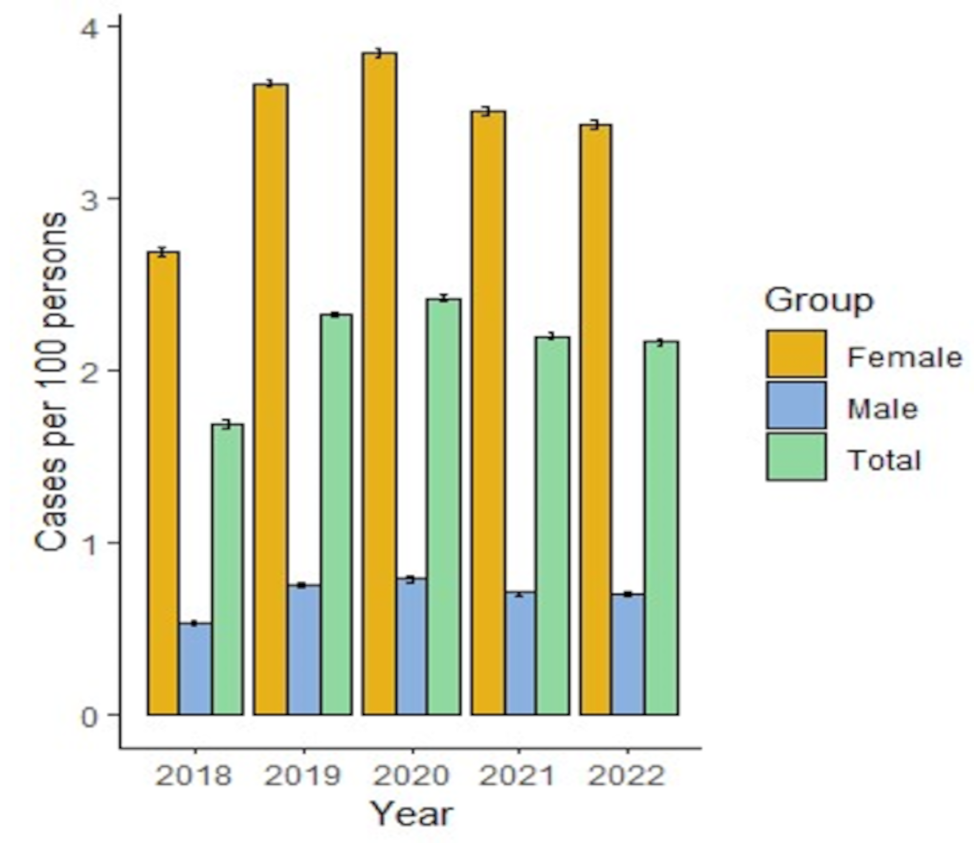
This is the first study to estimate the burden attributable to headache disorders in the adult general population of Morocco, the first in the Maghreb countries of North Africa, and the third of its type in EMR (after Pakistan [15] and Saudi Arabia [16]). It used the standard methodology and questionnaire developed by the Global Campaign against Headache [13, 14]. It found the symptom burden to be high: people with headache of any kind spent, on average, 12.5% of their time with headache of intensity rated 2.3 on a scale of 1–3. Females had significantly higher symptom burden than males. Average lost time attributed to headache was 0.5 days in 3 months from paid work, 1.6 days from household work and 0.3 days from social or leisure activities. Losses from paid work were considerably higher among males than females, a reflection of the low participation of women in the labour force in Morocco (among the lowest globally [21]). Losses from household work, on the other hand, were – as expected – significantly higher among females than males. A quarter of males (24.1%) and half of females (50.8%) with HY (17.8% of the sample) reported nothing or less than half done yesterday. At population level this diluted to an estimated 7.0% of all activity lost to headache.
These findings add to those on prevalence from our earlier study [17], informing health policy. In that study, we commented at length on the very high prevalence of migraine (30.8%) in comparison with the estimated global prevalence of 14–15% [22]. Inclusion of probable migraine was certainly a factor, and interest bias (mentioned again below) might have been [17]. Burden estimates at population level are, of course, to a large extent driven by prevalence estimates.
The high symptom burden at population level (8.6% of all time in the adult population spent with headache) is indicative of a high level of health-care need, but also offers the prospect of substantial improvement in population health through provision of health care to meet this need (effective treatments exist, and are cost-effective [23,24,25]). Our criteria for likelihood of benefit identified more than one third (36.8%) of the adult population of Morocco in need, a very similar proportion to the 35.8% we found in the Kingdom of Saudi Arabia [16] – despite the differences in culture, ethnicity and wealth. Half of those in Morocco (18.9%) were because of troublesome migraine (frequent and/or associated with substantially impaired participation) and more than one quarter (10.2%) were because of H15+. But 7.7% were because of TTH, either with pTIS > 3.3% and moderate or severe headache or with impaired participation in either paid or household work of > 3 lost days in 3 months. This last group need treatment, but, arguably, this need can largely be met by appropriate use of over-the-counter medications: that is, by health education and advice from community pharmacists rather than medical care. With these in place, health-care need would be reduced to about 30% of the adult population.
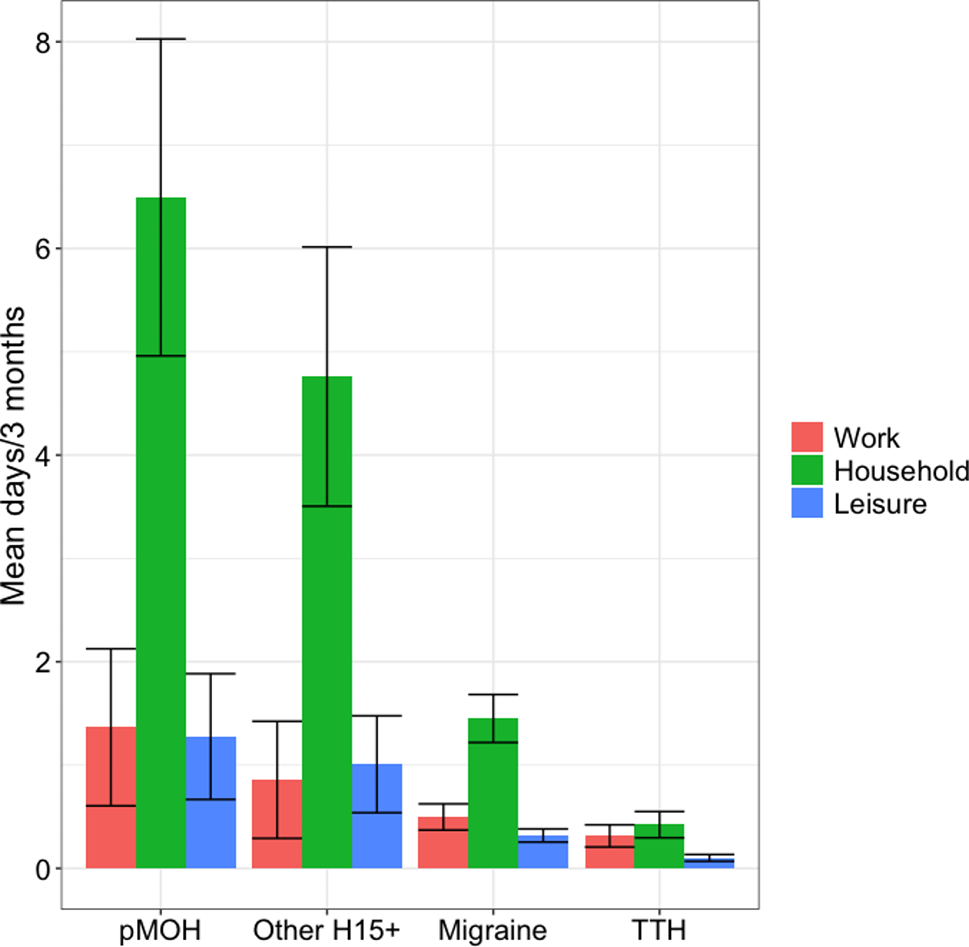
Our findings also inform economic policy in Morocco. Impaired participation estimates suggest that the health benefits of effective health care for those with disabling headache would be accompanied by the economic benefits of higher production. Means and medians were very far apart for lost-productivity findings (lost days from paid and household work), indicating a high level of skewedness, which suggests that a minority – who might be a priority target for health care –contribute disproportionately to population-level productivity losses. As expected, given the differences in symptom burden, higher productivity losses at individual level were attributable to migraine and H15 + than to TTH, and higher losses from paid work were attributable to H15 + than to migraine (Fig. 1). Nonetheless, while pMOH and other H15 + were associated with far higher pTIS than migraine at both individual and population levels, and were of similar intensity to migraine, it was migraine that was associated with the greatest productivity losses at population level. In other words, from an economic perspective, it is migraine that appears to be the priority target for health care. Migraine alone, it should be noted, was associated in those affected with the equivalent of a permanent diminution in health of 2.6%.
However, structured headache services – the suggested health-care solution to the burden of headache [23] – provide care not for specific headache types but for the full range of primary headache disorders, and MOH, and are cost-effective when priority is determined clinically rather than driven by expected economic benefit [24, 25].
This said, in many economies, structured headache services are potentially cost saving through recovery of lost productivity [25]. In Morocco, for migraine, pMOH and other H15+, productivity losses were greater from household work than from paid work, although significantly only for migraine (Fig. 1). This is unsurprising, since losses from household work were driven by females, among whom headache disorders were more prevalent. It is also the case that household work can, generally, be more easily deferred than paid work. However, household work means the necessary everyday chores of living, and its economic value should not be underestimated.
Recall error is a factor to be considered when disease-attributed burden is estimated from participants’ recall of symptoms and their effects on activities over past months. Accordingly, we made separate estimates based on yesterday (1-day recall) [13, 14]. With regard to population-level pTIS, the two estimates for all headache were similar: 7.2% based on HY and 8.4% based on long recall. This suggests our finding is reliable that the proportion of all time spent with headache in Morocco (among the population aged 18–65 years) is in this range 7.2–8.4%.
In contrast, headache-attributed impaired participation reported in association with HY (7.0%) was apparently much higher than impaired participation recalled over the preceding 3 months. But comparisons here were indirect. Impaired participation yesterday with HY was reported as how much, of planned activity, actually was not done, expressed as a proportion (%) without differentiating between different domains of activity. HALT-based enquiry, over the preceding 3 months, counted days lost in each domain separately, but it did not provide denominators for reliable calculation of proportionate losses. If it were assumed that, in 3 months, there were 65 days of paid work that could be lost, 90 days of household work and 90 days of social or leisure activities (allowing that, in any single day, activities might have been planned in all three domains), and if losses in the three domains were summed, the proportion would be 2.1% – much lower than the 7.0% estimated from HY data. But such assumptions would be untenable: the denominators are not knowable. For those engaged in paid work, denominators might be larger or smaller than 65 days, while denominators for household work and social or leisure activities might be (very much) smaller than 90 days. Further, in the HALT-based enquiry, participants were likely not to respond when an activity domain appeared irrelevant (for example, paid work for most females). We applied values of zero whenever data were missing (see Methods), so that individual-level averages were for all participants.
Therefore, the two methods of estimating impaired participation, rather than being discrepant, yield different information: absolute and relative. Lost productivity is better estimated from HALT data, but only in absolute terms: as average lost days per person (with or without headache). Overall impaired participation among the population (again including those with or without headache) is better estimated, as a proportion, from HY data.
As noted, data were collected during February to September 2019, which period included Ramadan (5 May to 4 June), in a country that is very predominantly Muslim. Dates of interview of each individual participant were not recorded, but about 12% of the data (one month out of eight) would have been collected during Ramadan. There is evidence that fasting is a cause of TTH-like headache [26], and, more specifically (although clinic- rather than population-based [27, 28]), that fasting during Ramadan has an aggravating effect on migraine, albeit, perhaps, only during the first 10 days [28]. Heightened awareness of headache during the fasting of Ramadan is also possible. Any such effects of Ramadan would have been captured in our study, with slight overemphasis (one month out of eight, rather than twelve). But these effects appear to be both small and uncertain, so that significant overestimation of overall burden is very unlikely.
The strengths of this study are that it was population-based, with an adequate sample size [14] (N = 2,575), and conducted in accordance with standardized methodology [13, 14]. While the sample had a high female-to-male ratio, statistical corrections for this were possible. Burden and productivity measures were assessed over short (1 day) as well as long time periods (weeks to 3 months) in order to rectify recall error.
Some limitations, previously noted [17], must also be considered. The failure of the interviewers to record refusals was a protocol violation. Their later recall of “up to 10%” cannot be relied on. Interest bias becomes likely when the non-participating proportion is large (> 10%), but, as noted previously [17], the observed 1-year prevalence of all headache (75.3%) was not unusually high. The necessary exclusion of the Fès sample because of the inappropriate method of sampling did not appear to have great impact on representativeness since the previously reported prevalence findings in this sample, with age- and gender-adjustment, were not greatly different from those of the main sample [17]. In cross-sectional studies with enquiry at a single encounter, further diagnosis of H15 + is limited to recognising its association with acute medication overuse (pMOH), or not (other H15+) [10, 11]. The diagnostic algorithm allowed only one diagnosis per participant, with migraine more likely to be diagnosed when both migraine and TTH were present. TTH-attributed burden might, therefore, have been somewhat underestimated. Resources were not available to validate the diagnostic question set within this study, but it had been validated in six earlier studies [15, 29,30,31,32,33] and used previously in 19 languages [13] including both French [34] and Arabic [10].


留言 (0)