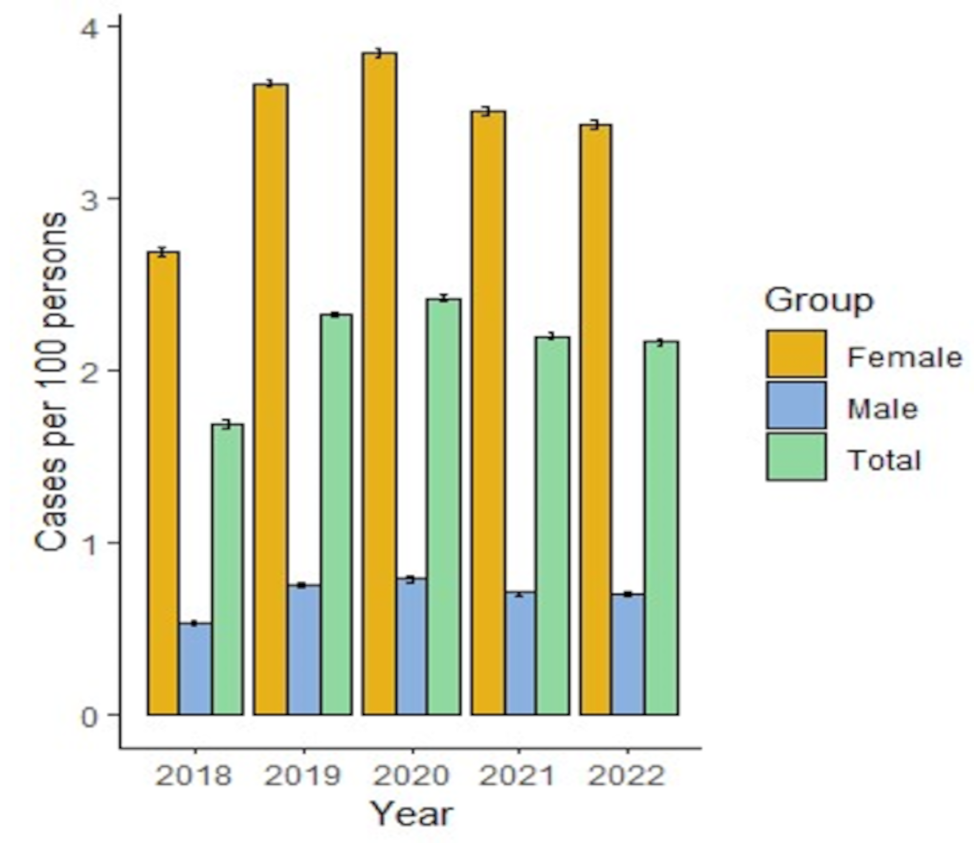
The results of this study, based on health electronic databases, show that the prevalence of migraine in Colombia from 2018 to 2022 varies between 1.69 and 2.42 patients in 100 affiliates, which is lower than that reported in other studies conducted in Latin America or Colombia. A wide variability in prevalence was found in previous studies conducted in Colombia [15,16,17]. Pradilla was found to have a prevalence of 7.1% (95% CI 6.5–7.7) in 1995–1996 using clinical examination based on World Health Organization protocols [15]. Morillo conducted a survey using the criteria of 1988 IHS in different countries, such as Colombia, in 1999, where the prevalence in females was 14.2% (95% CI 11.9–16.5) and that in males was 5.0% (95% CI 3.4–6.6) [16]. The most recent study was by Rueda [17], who also conducted another survey in a Colombian city using the Diagnostic Questionnaire for Migraine scale and reported a prevalence of 13.7% (95% CI 11.8–15.6). This heterogeneity is possibly related to the form of the prevalence estimation that depends on the study groups (such as hospital population and young people) or epidemiologists with interest in this disease, method used (e.g., nature of the screening question, number of conditions investigated, sampling method, number of participants), and case definition [18, 19]. This study provides real-world evidence using the electronic health databases of one insurance company with approximately 5 million affiliates. Russell et al. defined it as administrative prevalence, which suggests that its variability, compared to that of populational studies, is caused by self-medication of patients who did not see a health care professional after initial diagnosis or who were able to treat their episodes due to the low frequency of attacks [13]. Additionally, according to a study by Eurolight in Europe, 15.8–33% of the population with migraine consulted a health care professional [20], and Morillo reported that 50.9% of patients did not consult a health care professional [16].
The incidence of migraine in Colombia was similar to that estimated by the Global Burden of Disease Study in 2019, in which for Andean Latin America, the age-standardized rate was 0.9 (95% CI 0.7–1.2) per 100,000 individuals aged 15–39 years, and that for Central Latin America was 1.3 (95% CI 1.1–1.7) per 100,000 individuals [19].
Both the incidence and prevalence were higher overall in the female and young adult age groups (18–24 and 25–34 years). This finding is similar to that described by Pacheco et al. [4] in a systematic review, which suggested that females had a four-fold greater chance of having migraine than males did (12.78%, 95% CI: 9.19–16.85 vs. 3.50%, 95% CI: 2.47–4.69). However, Morillo reported that the prevalence was higher in individuals aged between 30 and 39 years. 40–49 and 50–59 [16]. Pradilla reported the highest frequency of migraine between the third and fourth decades of life [15]. Other studies suggest that the prevalence increases in the young adult population until approximately age 40, then the prevalence starts to decline, which is similar to the trend observed in this study [21].
In contrast with a previous review [19], we found a decrease in the incidence of migraine since 2020, which may be related to environmental factors, strict diagnostic criteria, or patient preference for not consulting health care professionals during the COVID-19 pandemic. It has been argued that governmental measures related to the COVID-19 pandemic, such as the impact of lockdown on patients with migraine, may be modified by lifestyle and behavioral factors, as well as transformed or limited by healthcare [22]. However, currently published studies on headache in the setting of COVID-19 have concluded that some outcomes may increase or decrease the burden of disease, considering that headache-attributed burden not only has multiple and diverse components but is also very unevenly distributed in populations with current migraine [18, 22].
The frequency of cardiovascular conditions in migraine patients observed in this study was higher than 20% of the population due to essential hypertension. Additionally, the prevalence of hypercholesterolaemia and diabetes mellitus is between 5% and 10% in this population. Some studies have suggested that hypertension, dyslipidemia, and diabetes mellitus are considered risk factors for migraine [23]; however, these studies have yielded conflicting results, and the associations have not been validated [21, 24, 25]. The frequency of cardiovascular disease was similar to that reported in other studies in the United States [7] and Israel [26]. According to the Dodick study, which has similar data sources to those used in this study, the main cardiovascular diseases were ischemic cerebrovascular disease, structural heart disease, arrhythmias, uncontrolled hypertension, and ischemic heart disease, which accounted for less than 6.8% of the population [7]. On the other hand, these medical conditions are considered warnings for migraine patients, especially those receiving triptans, where treatments are limited to NSAIDs, nonopioid analgesics, and caffeine analgesic combinations [7]. However, the long-term use of NSAIDs increases the risk of myocardial infarction and stroke, hypertension, peptic ulcer disease and bleeding, and nephrotoxicity, especially in older adults [27,28,29].
According to the study, NSAIDs, corticosteroids and combinations of other analgesics were the main medications used for acute treatment. Triptans were used in lower proportions, but their use increased over time. This behavior is analogous to that observed in the study by Roessel et al. that was conducted in Germany, where NSAIDs were also more frequent, but they were characterized by ibuprofen and metamizole. Additionally, in the same study, corticosteroids were used as emergency medications [13]. In studies conducted in the United States, triptans were used more than to manage episodic migraine in more than 50% of patients, and rizatriptan and sumatriptan were the most commonly used triptans [30, 31].
Opioids were used in lower proportions in this study than in previous studies in Germany (19.1%) and the United States (8.3 − 53%); however, opioid use for more than 90 days was observed in more than 40% of patients. Another study in Colombia reported that almost 7% of patients were managed with tramadol [32], which is very similar to what was observed in this study. These findings are relevant given that the evidence of the efficacy of opioids is low or insufficient and that opioids are associated with increased rates of gastrointestinal-related adverse events, addiction, and drug abuse secondary to the treatment of migraine [33, 34]. For that reason, guidelines recommend against the use of opioids in the management of acute migraine [35, 36]; nevertheless, the use of opioids was observed in a high number of patients. Moreover, the use of opioids for acute migraine therapy after other analgesics or chronic use can indicate that patients need more efficacious treatment for migraine. Additionally, the persistence of episodic migraine was low during the follow-up period. NSAIDs were switched with another treatment in more than 50% of patients at 90 days of treatment and in more than 80% of patients during the year of follow-up. There was a lower proportion of patients who switched from treatments with triptans than other analgesics, but 50% of patients changed at 267 days, and almost 60% changed at the year of follow-up. This low persistence is another index to indicate the unmet needs of patients for more efficacious treatments, as mentioned before.
For preventive medications, the findings of the German population study by Roessler et al. were similar to those for beta-blockers, but metoprolol was the most frequent. Additionally, the use of anticonvulsants was also lower than that in the Colombian cohort, where antidepressants stand out. The use of onabotulinum toxin A was reported in only 0.8% of patients [13]. In the Ford et al. study, preventive treatment was used for 52% of episodic migraine patients and 95.6% of chronic migraine patients, where topiramate was the most frequent. Beta-blockers were reportedly used in only 8.0% of the population [31]. Woolley et al. reported that 65% of migraine patients did not receive preventive medications. Topiramate was the most frequent follow by beta-blocker and tricyclic antidepressants [30]. Moreover, the persistence of preventive medications was greater in the Colombian cohort, in which the median duration until patients required a switch was greater than 180 days, while in the Woolley cohort, it was 90 days [30].
Another common treatment has been ergotamine with its different combinations, mainly caffeine. According to this study, it was used in 20.5% in first visit with decreasing trend for subsequential visits. Based on a Colombian study that analyzed the appropriate use of ergotamine according to guidelines and medical interactions found that the 98.5% of prescription were unappropriated [37].
Another study conducted in Colombia in a cohort of 241 patients revealed that propranolol was the most commonly used treatment, followed by valproic acid and amitriptyline [38], which followed the same trend as the one in this study. Both Osorio et al. and this study observed treatments recommended by the American Headache Society (AHS) and the American Academy of Neurology (AAN), where topiramate, valproic acid, metoprolol, and propranolol are recommended for preventive treatment, and are supported by a high level of evidence [39]. CGRP monoclonal antibodies have been reported in very low proportions, possibly because of their recent availability on the Colombian market and their high cost compared to other treatments. These medications have been studied in Colombian patients under common practice assessing the clinical outcomes, however, the sample size was small [40]. Another important treatment is onabotulinum toxin A, which affects a wide group of patients every year and has adequate persistence.
This study intended to evaluate the persistence of acute and preventive treatment which vary between 85 and 311 days depending on treatment and other clinical patient characteristics. Persistence could consider a gross measure of effectiveness, however, it could be affected by other characteristics. An study conducted in Portugal evaluating the efficacy of preventive treatment found that it was 40% which was decreasing in successive prophylactic attempts. Additionally, it observed high percentage of dropout [41].
According to this study, the management of patients with migraine is mainly conducted by general practitioners, and a low proportion of patients with migraine are managed by neurologists or emergency specialists. This finding is similar to that of a previous study in Colombia by Morillo [16], which was conducted in 1999, implying that the management of migraines did not undergo major changes after 20 years. In Germany, the results of this study were very similar to those of other studies in which management was led by a general practitioner; however, neurologists participated more than in Colombia [13]. However, in a United States cohort, neurologists were more involved in the management of migraine than in the Colombian cohort, and managed 30% of patients with episodic migraine and 65% of patients with chronic migraine [31]. However, the number of consultations was very similar to that in Colombia, where there were 1.9 to 2.8 days of consultations per year. The frequency of hospitalization was 3.6% according to Ford et al. [31], but in this study, it was 0.1%.
This study is the first in Colombia to analyze electronic health databases, including medical records, claim databases and laboratories. One strength of this study is that it can analyze a large number of patients from almost 20% of the contributive regime in Colombia, which increases the representativity of the Colombian population. The information of the HMO allows us to register all care that affiliates receive, including the supply of treatment, hospitalization, or medical consultation. The patients who were selected for inclusion in the analysis were confirmed by physicians or clinical specialists, which decreased misclassification bias and allowed us to guarantee the accurate characterization of patients with migraine. Additionally, five years of analysis of the cohort was feasible for the organization and management of the data by the HMO; thus, any variation in the cohort during the follow-up made it possible to analyze and decrease any bias due to secular tendencies.
Our study is the most comprehensive to report on migraine epidemiology in Colombia. Although it does not reflect the true prevalence of the disease, this study provides valuable information for clinicians and national policy-makers, presenting the burden of migraine in the health care system and providing a basis for decisions on health resource allocation.
This study has some limitations due to the nature of the study and the availability of information. The first filter of the study was limited by the use of the ICD-10, in which patients for whom the physician was not adequately registered were excluded from the study. The sources of data used in this study are widely used and validated for reporting the outcomes described. However, databases have limited records since they can suffer from omissions, site-specific coding problems, coding bias, incorrect coding, and insufficient detail in the characterization of disease chronicity. This was mitigated with the parameterized collection of the variables established in the protocol. The options for the variables were predefined in accordance with the availability and structure of the site data. Another limitation is the risk of patients having a combination of episodic and chronic migraine, given that patients can be diagnosed by other insurance companies and that insurance companies can change during follow-up. There was an important group of patients who were lost to follow-up given that they claimed treatment and that there was no registration of other care for other episodes of migraine in the health care system. Finally, patients who were self-medicated or had migraines without a diagnosis were not included in this study, reducing the representativeness of the study.


留言 (0)