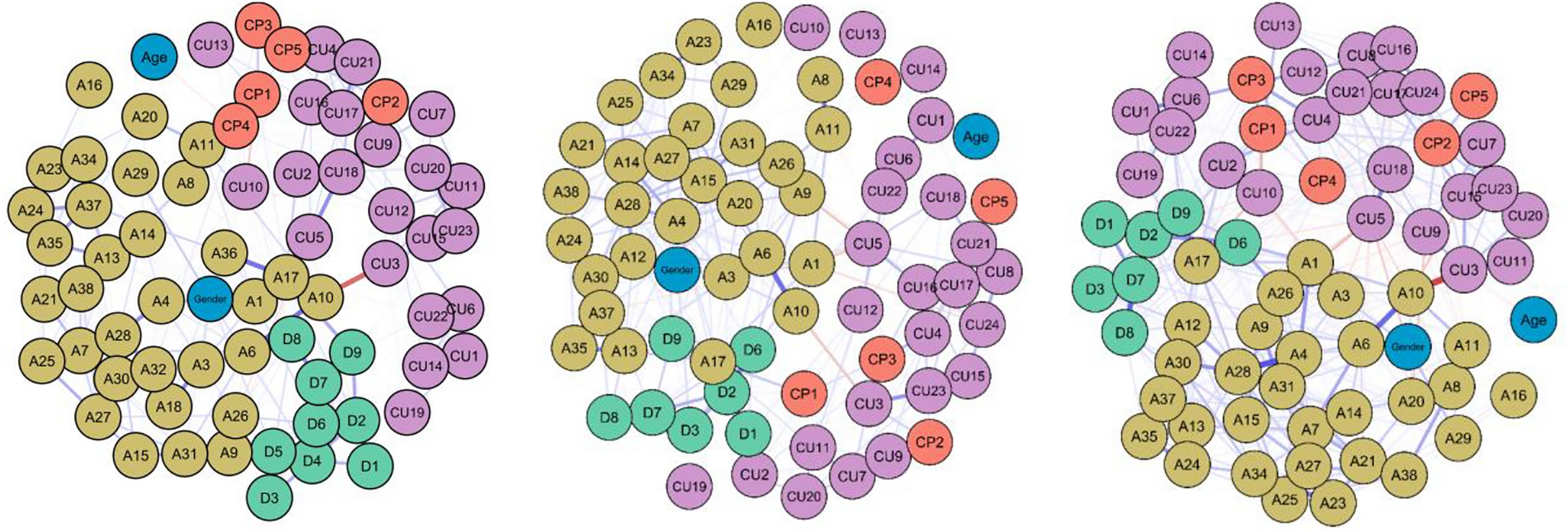
The present study applied network analysis to conceptualize the role of callous-unemotional (CU) traits in internalizing psychopathology in adolescent psychiatric inpatients. In step one, a network of CU-traits, internalizing symptoms (i.e., depression, anxiety), and externalizing symptoms (i.e., conduct problems (CP)) was analyzed within 978 inpatients with a range of psychopathological conditions (network analysis 1). In step two, the network was compared between individuals with conduct disorder (CD) and individuals with internalizing (INT) psychopathology (network analysis 2).
Core symptoms of the CU-INT comorbidity network
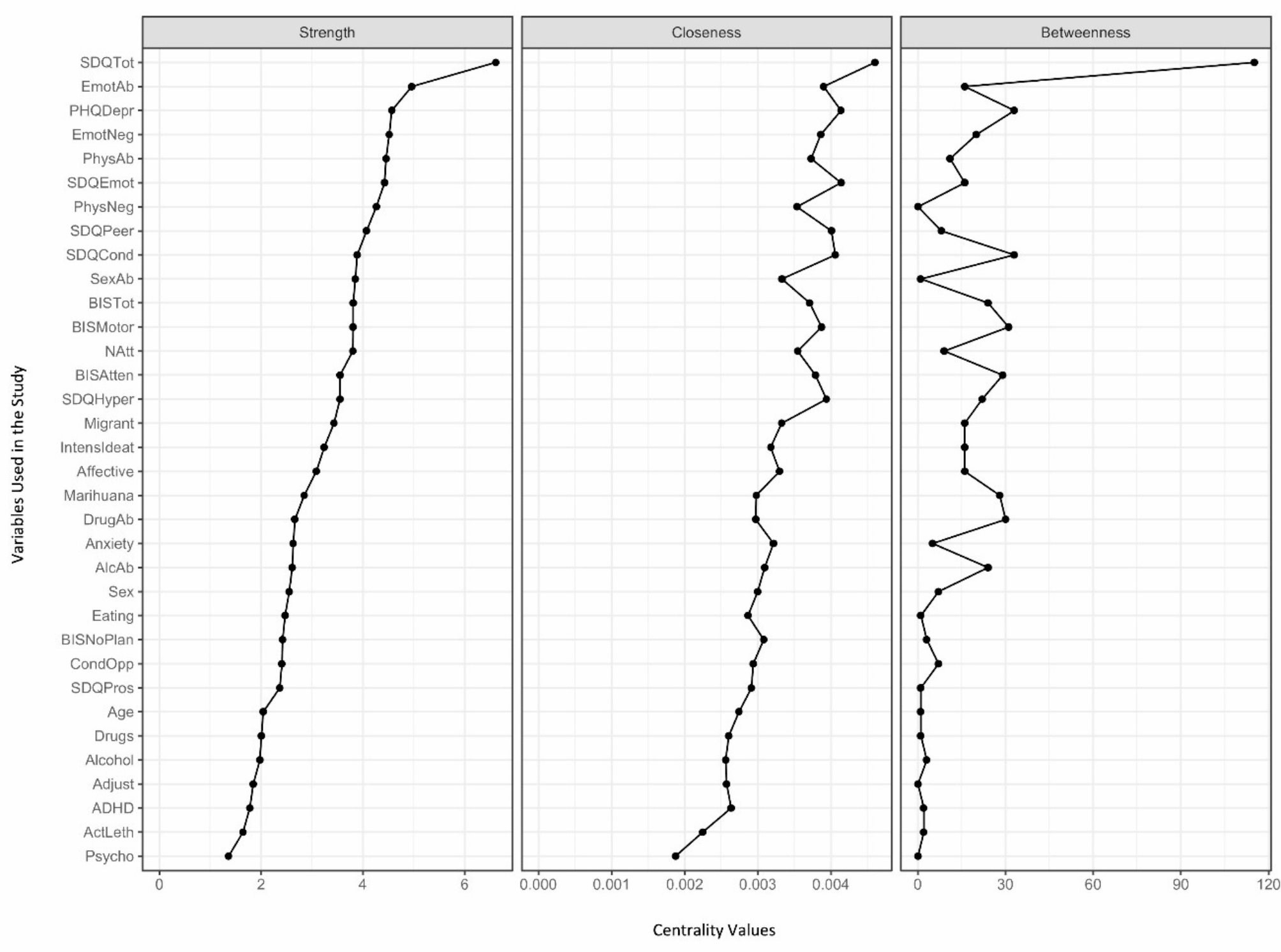
This study aimed to identify the most central symptoms within the combined network of CU-traits and internalizing psychopathology. Depressive symptoms (i.e., depressed mood), anxiety symptoms (i.e., sudden fear, feeling afraid, obsessive thoughts, worry about school performance), and CU-symptoms (i.e., uncaring about hurting others, not showing emotions) emerged as core symptoms. The centrality of depressed mood might be explained by the fact that half of the sample had a diagnosis of depression as the main diagnosis, and depressive symptoms also co-occur frequently with other diagnoses [53].
Surprisingly, depressed mood remained the only depression item among the most central items, whereas anxiety items played an especially prominent role. This might be explained by the high degree of comorbidity between depression and anxiety disorders [54] and the transdiagnostic nature of questionnaire items. Whereas sudden scare and feeling afraid are typical symptoms of anxiety disorders, worrying about school performance, as well as obsessive thoughts are rather transdiagnostic symptoms. For example, worrying about school might also result from concentration problems and lower performance levels typically associated with depression [55] or substance abuse disorders [56] or from disruptive behavior problems typically occurring in CD [57]. Although the item regarding obsessive thoughts is meant to measure obsessive thoughts occurring in obsessive–compulsive disorder, the item is framed in rather general language. Thus, depressive patients might experience suicidal thoughts as obsessive, whereas, for example, youth with substance abuse might experience thoughts about taking drugs as obsessive. Worrying or rumination about a certain topic might, therefore, be a transdiagnostic symptom rather than a pure anxiety symptom.
Rather surprisingly, two CU-items were among the most central nodes. The first CU-item, not showing emotions, points to a connection between the unemotionality facet of CU-traits and internalizing symptoms. Within (primary) CU-traits, unemotionality is regarded as a trait present from birth and is already observable in 6-month-old babies [58], accompanied by deviations at the neural level (e.g., reduced amygdala activity toward emotional stimuli; [59]). In this concept, unemotionality refers not only to expressing emotions but also to not experiencing emotions as strongly (e.g., lessened threat reactions [6] and reduced affective empathy [3]). The item, however, measures not showing emotions more generally. Youths with depression [60, 61], social phobia (e.g., [62]) and CU-traits [1] all seem to have diminished emotional expressions; however, the reasons underlying this facet of unemotionality possibly differ strongly between the diagnostic categories. Whereas adolescents with social phobia might show less emotional expression to avoid interaction and due to an internal state of fear [63], diminished expression in depressed individuals may serve the purpose of inhibiting ongoing emotional reactivity in adverse and potentially dangerous environments [64]. Thus, not expressing emotions can be regarded as a transdiagnostic symptom that occurs in diverse psychopathologies, and this transdiagnostic mechanism could potentially help explain the results of studies finding positive associations between measures of CU-traits and anxiety and depression [15, 16].
The relevance of the second central CU-item, uncaring about hurting others, seems counterintuitive at first glance. Although correlations with other CU-symptoms and with CPs seemed likely, associations with depressive and anxiety symptoms were rather unexpected. An explanation might be the concept of a secondary variant of CU-traits [20]. In patients who experienced a high number of adverse life events, CU-traits and internalizing symptoms may have developed comorbidly in response to adverse experiences. In patients with primary CU-traits, however, no associations or negative associations with internalizing symptoms might arise. Independent of their origin (primary or secondary pathway), the CU-traits expressed by patients are theoretically thought to be the same (for conflicting evidence, see [65]). The ICU, which was employed in the present study, cannot differentiate between the variants. Yet, the high number of internalizing diagnoses in the total sample (i.e., more than half of the participants had a primary diagnosis of depression) makes the presence of secondary CU-traits more likely. These secondary CU-traits might drive correlations between CU-traits and anxiety or depressive symptoms, resulting in a relatively high centrality of CU-symptoms.
Transdiagnostic mechanisms between anxiety, depression, and CU-traits
In the network analysis, losing temper and lying/cheating emerged as relevant bridge symptoms, or transdiagnostically relevant symptoms, in the CP-cluster. Within the anxiety cluster, obsessive thoughts were the most important bridge item. Within the depression cluster, psychomotor functioning and suicidal ideation were the most important bridges. With respect to CU-traits, uncaring about hurting others was also a bridge item, together with feeling guilty*. CU-traits did not have substantially lower bridge values than the other clusters did. The bridge strength value was even greater for some CU-items than for depression items. This result seems to provide evidence for a potentially transdiagnostic mechanism of CU-traits. With respect to CPs, CU-traits seem to be a risk factor: There were positive bridges between not feeling guilty* and obedience* and between uncaring about hurting others and fighting/forcing others, which fits well with the literature [3]. For anxiety and depressive symptoms, the picture was more complex. Feeling guilty* seemed to be a protective factor as it has negative bridge associations with worrying and depressed mood. This finding is consistent with the literature showing that guilt is positively associated with internalizing disorders and negatively associated with externalizing disorders [66]. In contrast, uncaring about hurting others may be a risk factor for the activation of psychomotor functioning and checking behavior through positive bridges. One reason for this might be the hyperarousal found in adolescents with high CU-traits and high comorbid internalizing psychopathology (i.e., secondary CU-variant) [20]. Checking behavior might be a strategy to cope with hyperarousal and associated stronger responses to socioemotional stimuli. Psychomotor functioning captures slowing down or being restless. Restlessness might also be a symptom of the hyperarousal associated with secondary CU-traits.
Comparisons of the CD- and INT-networks
The results of the network comparison between the CD- and INT-subsamples were contrary to our expectations. We expected the CD-network to be denser than the INT-network, as indicated by strength invariance. We also expected CD and CP nodes to be especially central in the CU-network, and depression and anxiety to be especially prominent in the INT-network, expressed by centrality invariance. Instead, our results all pointed in one direction: CU-traits were relevant in both networks. Moreover, the INT-network had a greater density (i.e., greater connectivity among symptoms) than the CD-network. Based on the literature, one would expect that the higher density scores might be explained by stronger edges between anxiety and depressive symptoms owing to their symptomatic overlap and comorbidity [53] in internalizing samples. However, most of the variables that were significantly more central in the INT-network were CU-nodes. These CU-items included symptoms from all three CU-facets: unemotionality, callousness, and uncaringness. This surprising finding fits well with the model of secondary CU-traits and is in line with previous findings of increased anxiety and depression in this patient group [15]. Interestingly, CD seemed to have an impact on these relations: Within the CD-network, CU-symptoms exhibited mostly positive associations with CPs and depression symptoms but negative associations with anxiety symptoms. This matches the pattern associated with primary CU-traits (e.g., [4]). In contrast, in the INT-network, only a few (mostly negative) pathways were observed between CU-traits and anxiety symptoms, which shows that CU-traits and anxiety might be unrelated in INT-samples. This was also reflected in the edge invariance test that pointed to significant differences among CU-internalizing pathways between the networks. The results are consistent with the contradictory findings in the literature that have established positive associations between CU- and internalizing symptoms (e.g., [15]), no associations (e.g., [9]), or negative associations (e.g., [4]). The data further show that depression and anxiety should not be combined when looking at associations with CU-traits.
Translation to psychopathology and psychotherapy
Our results contribute to the current understanding of the architecture and transdiagnostic role of CU-traits. CU-items were central and influential not only in the CD-network but also in the INT-network and the overall transdiagnostic network—even when controlling for CPs, age, and gender. Interestingly, items from the unemotional facet of CU-traits were not the only ones associated with internalizing symptoms. Items from the callousness and uncaringness dimensions of CU-traits also served as bridges between the disorders. This finding extends the results from previous network analyses that identified these dimensions as bridges to externalizing symptoms [28, 29], highlighting their relevance for internalizing symptoms as well.
The network comparison pointed to somewhat differential associations of CU-traits and internalizing symptoms between the CD- and INT-patient groups. These divergent results might be related to differences in CU-variants: primary and secondary CU-traits, respectively. Whereas the CD-network might have contained a higher proportion of participants characterized by primary CU-traits, the INT-network might have contained a higher proportion of participants with secondary CU-traits. As the ICU used in this study to measure CU-traits does not account for the aetiology of CU-traits, further studies are needed to shed light on this hypothesis. In sum, our results point to the relevance of CU-traits across diagnostic categories in line with the previous work of Herpers and colleagues [67], rather than having relevance only for externalizing behavior problems, as proposed by Frick and Moffitt [68]. Clinically, our results have implications for psychotherapeutic approaches within CU-traits. CU-traits are traditionally only targeted in the treatment of externalizing patient groups; however, our results imply that it might be helpful to address CU-traits in the treatment of internalizing patients. There is accumulating evidence (for a review, see [20]) that adolescents who are high on both CU-traits and internalizing psychopathology are at higher risk for adverse outcomes. Therefore, studies should investigate the effects of including CU-traits in treatment programs for internalizing patients.
Comorbidities traditionally present a challenge for clinicians because they have a negative impact on treatment success, and it is often unclear which symptoms should be prioritized during treatment. Central and bridge symptoms might be a reasonable choice to address first in treatments because targeting them may disrupt pathways that maintain comorbidity and spread across several symptoms [24, 69]. Our results suggest that when combining results regarding node and bridge centrality, clinicians should focus especially on the anxiety item obsessive thoughts. This item was among the items with the highest (bridge) centrality and was the only node in the network nominated in all categories. Furthermore, no difference in the centrality of this node between the subsamples was found, indicating an equally high relevance of this item in both subgroups. As mentioned above, it remains unclear whether the high centrality of obsessive thoughts is due to the wording of the item, which might capture very different types of thoughts experienced as obsessive (e.g., suicidal or negative thoughts in depression, thoughts about substances in addiction, or thoughts about a specific anxiety-related stimulus in phobic disorders). If the item captures worrying or rumination, as speculated, then the current results match results from another network analysis in an adolescent clinical sample: in Ruan et al.’s [35] network analysis, worrying was established as an essential bridge between anxiety and depression. Further studies are needed to investigate whether obsessive thoughts are also central to other symptom networks in adolescent psychiatric samples.
Limitations
The present study has several limitations. The sample was not equally balanced across the categories of anxiety, depression, CPs, and CU-traits. Whereas approximately half of the sample had a primary diagnosis of depression, less than one-fifth of the participants had a primary diagnosis of CD, and only a small number of participants suffered primarily from an anxiety disorder. Additionally, our sample was highly comorbid and had a high level of psychopathology in general, as we recruited psychiatric inpatients. The study has been conducted in Germany, which might have implications on the sample's composition in terms of the most prevalent diagnostic categories. Symptoms were assessed via self-reports, which might be more reliable for internalizing (depression, anxiety) than for externalizing (CP, CU) symptoms [70] and might be biased by the participants’ current emotional state. Future studies should include a more balanced sample regarding internalizing and externalizing disorders. Symptoms should be assessed with multi-informant reports.
The data collected in the study are cross-sectional. Therefore, we cannot make any statements regarding the causality and predictive value of the results. The identified bridge and core symptoms may be influenced by other symptoms, actively influence other symptoms, or both within the causal chain. Future studies should assess symptoms longitudinally to obtain a clearer understanding of developmental trajectories among symptoms.
The groups compared with the network comparison test had unequal group sizes. Therefore, the results for the INT-group have more statistical power than those for the CD-group. Future studies should recruit more patients for both groups. Finally, we cannot generalize our findings across cultures or age groups, as this was not a multicenter international study that spans the lifespan.

留言 (0)