Participants
Forty-six inpatients between 10 and 14 years of age diagnosed with CD based on the International Classification of Diseases (10th ed.; F90.1, F91.-, F92.-; [28]) were recruited from the LWL-University Hospital for Child and Adolescent Psychiatry Hamm in Germany. The exclusion criteria were an IQ < 85 or disorders that impaired the ability to participate in the study (e.g., acute psychosis, acute suicidality). Of the 46 participants, six had to be excluded from the analysis for various reasons: hospital discharge before conducting the VR-task (n = 1), turning 15 years old in between screening and testing (n = 1), lack of a CD-diagnosis in a clinical screening interview (n = 1), technical problems during the VR-task (n = 3), resulting in a CD-sample of n = 40.
In addition, 32 TD-children were recruited from high schools in the Hamm area. Of the 32 participants, one had to be excluded from the analysis due to an IQ < 85, and another due to technical problems with the VR-task, resulting in a TD-sample of n = 30. The total sample of the study comprised n = 70 participants (Mage = 12.5, SD = 1.39). The study was approved by the local medical-ethical committee (Ruhr University Bochum, Nr. 20-6861; 18th May 2020).
MeasuresCU-traits
In light of studies pointing to informant discrepancies on internalising as well as externalising symptoms [29], especially in adolescence and for social avoidance [30], we chose to assess parent- as well as self-report on CU and SA. While there was a significant and positive correlation between parent- and self-report for CU-traits (Spearman’s ρ = 0.323, p =.009), no significant association was found for SA (Spearman’s ρ = 0.109, p =.388). Therefore, both reports were included in the analyses of the current paper
CU-traits were measured with the German parent- and self-report versions of the Inventory of Callous-Unemotional Traits (ICU; [31]). The ICU contains 24 items scored on a 4-point Likert scale ranging from 0 (not at all true) to 3 (definitely true). The items describe indifference in relation to one’s own performance and feelings of others, lack of guilt, empathy, and remorse, and reduction or absence of emotional expression. By adding up all items, a total score can be derived. In the current sample, reliability was excellent for the parent-reported total score (Cronbach’s α = 0.90) and good for the self-reported total score (Cronbach’s α = 0.81).
Social anxiety
SA was measured with the German parent- and self-report version of the Social Anxiety Scale for Children - Revised (SASC-R-D; [32]). The SASC-R-D consists of 18 items scored on a 5-point Likert scale, ranging from 1 (never) to 5 (always). The items describe fear of negative evaluation as well as social avoidance and distress in various social situations. By adding up all items, a total score can be calculated. In the current study, the reliability of the total score was excellent for parent-reports (Cronbach’s α = 0.91) and for self-reports (Cronbach’s α = 0.92).
Intelligence screening
IQ was measured with the short version of the Wechsler Nonverbal Scale of Abilities (WNV; [33]). The WNV is a nonverbal measure of ability for children and adolescents aged 8–21 years. The short version consists of the two subscales “Matrices” and “Spatial Span”, and a total IQ score can be derived.
Structured diagnostic interview
The Diagnostic Interview for Children and Youth for DSM-5 (Kinder-DIPS, DSM-5 version; [34]) is a structured clinical interview to assess common mental disorders in childhood and adolescence based on DSM-5 criteria. The DIPS was completed with participants’ legal guardians.
General psychopathology
General psychopathology was measured with the Child Behaviour Checklist (CBCL/6-18R; [35]). The CBCL is a parent rating scale assessing behavioural problems, emotional problems, somatic complaints and social competences of children and adolescents with 113 items. A total score as well as scores for the subscales “internalising” and “externalising behaviour problems” can be derived. In the current study, Cronbach’s α = 0.94 for the total score, 0.86 for the internalising subscale, and 0.91 for the externalising subscale.
Visual analogue scales
Mood was rated on five 10 cm long visual analogue scales (VAS; e.g., [36]) ranging from 0 (not at all) to 100 (very) based on the five emotions (i.e., neutral, happy, angry, sad, anxious) used in the virtual IPD-task.
To control for the possible influence of the outbreak of the pandemic shortly before the beginning of the study, two VAS were used. Participants were asked to rate (a) “What do you think, how much does the COVID-19 pandemic influence your behaviour at the moment?” and (b) “What do you think, how much has the COVID-19 pandemic influenced your behaviour in the VR-task?” on a 10 cm sliding scale ranging from 0 (not at all) to 100 (very much).
Virtual interpersonal distance task
Automatic approach and avoidance tendencies were measured with a virtual reality (VR) task. For this task, a virtual environment resembling a school cafeteria was created (see Fig. S.1). Participants wore a stereoscopic head-mounted display that immersed them in the VR-scenario and signalled the participant’s physical position and orientation in the room to the computer (15 Hz) to adjust the displayed scene accordingly. Participants had the ability to walk around freely. The research lab had objects (tables and chairs) located at the same locations as in the VR-environment to increase the immersiveness of the virtual world. Immersiveness was further strengthened by typical cafeteria acoustics (e.g., voices, clattering crockery).
General task setup. During the task, the participant encountered a virtual agent in a school cafeteria. A cover story was used, which included the agent being a new classmate whom the participant would meet for the first time at the school cafeteria during a lunch break. On each trial, the participant stood with his back toward the agent behind a yellow starting line at 5.3 m away from the agent. The participant was instructed to turn to the agent after an acoustic signal (the agent said hi/hey/hello; prerecorded with real children’s voices). The participant was then supposed to walk toward the agent. The agent’s age and height were adapted to the participant’s age and height. The agent’s body was oriented toward the participant’s starting point and during the trial, his head moved to maintain an orientation toward the participant. After completion of the trial-specific task, the participant was instructed to return behind the yellow line. When the participant stood with his back to the agent behind the starting line again, the next trial with a new agent started. For the task, different virtual agents (see Fig. S.1) were created that appeared in a randomized order. Throughout all trials, the agents displayed a nonspecific greyish eye colour that changed gradually with the approach of the agent; the change started at 1.5 m away from the agent and was finalized at 1 m from the agent to ensure that participants walked close enough to the agent and paid attention to the facial region. The complete VR-task lasted for approximately 15–20 min. The minimal distance participants held to the agent (interpersonal distance, IPD) on each trial and the walking speed (WS) while approaching of the agent were the variables of interest recorded during the task.
Practice trials. The task started with three practice trials in which the participant encountered a virtual robot to become acquainted with the task setup and the VR-environment. The participant was instructed to recognize the robot’s eye-colour and walk back behind the yellow line after each eye-colour recognition.
Indirect trials. During these trials, virtual agents were boys introduced as new classmates. The task was the same as in the practice trials: participants were instructed to recognize the virtual classmate’s eye colour. The indirect phase consisted of 23 trials: (1) one practice trial with a virtual classmate maintaining a neutral emotional expression throughout the whole trial, (2) four trials with a neutral emotional expression, (3) two emotional practice trials with a task-irrelevant emotion (disgust), and (4) 16 emotional trials (4 emotions X 4 repetitions) with task-relevant emotional expressions (i.e., anger, anxiety, happiness, sadness) in a randomized order. The same emotion was never presented more than twice in a row. All emotional trials started with the agent displaying a neutral facial expression that gradually changed into a distinct emotional expression during approach. The change started at 4 m from the agent and was finalised within 2 s (or at latest 3 m) from the agent.
Direct trials. The direct phase consisted of four emotional trials in which different agents showed every task-relevant emotion once. Participants were instructed to approach the agent up to a distance where they found it comfortable to begin a conversation. Then they were supposed to greet the agent loudly, again imagining that they met a new classmate in their school’s cafeteria.
Emotion recognition
Explicit emotion recognition (ER) was tested with a computerized emotion recognition task (ERT) to check whether participants were able to identify the emotional expressions shown by the virtual agents in the VR-task. Participants were presented with screenshots of the full-blown emotional expressions (i.e., neutral, happy, angry, anxious, or sad) of the agents in the VR-task on a standard lab-computer. The face appeared in the middle of the computer screen and had to be categorised to the respective emotional label. Participants had to categorise 25 faces (5 expressions X 5 repetitions; see Figure S.2).
Procedure
All information, questionnaires, and instructions were presented in German. Patients admitted to the hospital with a CD-diagnosis and their parents were contacted for the study. Healthy controls were recruited at local schools through information events, flyers, and posters in public places. Potential participants and their legal guardians were informed about the study verbally and in writing and were given the opportunity to ask questions. After informed consent was received, the Kinder-DIPS was conducted with legal guardians for screening purposes. For the control group, the entire Kinder-DIPS was administered to ensure that the child did not suffer from any clinically relevant mental disorders. For the patient group, the diagnosis of CD was verified by assessing the respective conduct disorder sections of the Kinder-DIPS. After that, legal guardians completed the parent-report questionnaires (ICU, SASC-R-D, CBCL).
Participants were tested in individual sessions at the clinic’s VR-lab. For patients, testing took place in the morning prior to taking medication to minimize drug effects. The WNV was conducted with participants if no prior IQ-measurement had taken place within the previous half year. After completing the self-report questionnaires (ICU, SASC-R-D)Footnote 1 and mood-VAS, participants were asked to execute the VR-task. Testing ended with the ERT and the Covid-VAS. The participants were thanked for their participation and rewarded with sweets. Controls received an additional small compensation for coming to the clinic’s VR-laboratory. No debriefing took place to prevent other potential participants from knowing about the real study goal.
Data preparation and statistical analysis
VR-trials in which the researcher observed irregular behaviour of the participant (e.g., turning around on the way to the agent, stopping halfway to pose a question, or changing position of the VR glasses) were excluded from the analysis (nipd = 60, nws = 70). Additionally, for the indirect phase, trials were excluded from the IPD analyses if the IPD was less than 20 cm from the agent because with an IPD below 20 cm, the participant is likely to have walked into the agent and therefore did not adhere to the task instructions. This resulted in the exclusion of 21 trials (1.5% of trials). One participant was excluded completely from the analysis of indirect trials as nearly half of his trials had to be deleted due to extremely low IPD-values. Missing values on questionnaires were analysed and found to be missing completely at random (Little’s MCAR test: chi² = 537.12, p =.104). Missing data were replaced with the individual mean value on the respective questionnaire’s subscale. The ER-task had very few missing responses (0.4% of trials) which were not replaced as the percentage of correct responses was not dependent on the number of times a specific emotion was rated.
IBM SPSS Statistics 29 was used for the data analysis. Descriptive statistics were calculated for the variables of interest. Differences between groups with regard to all descriptive measures, ER error rates, VAS, and demographics were assessed with two-tailed independent samples t-tests or chi-square tests.
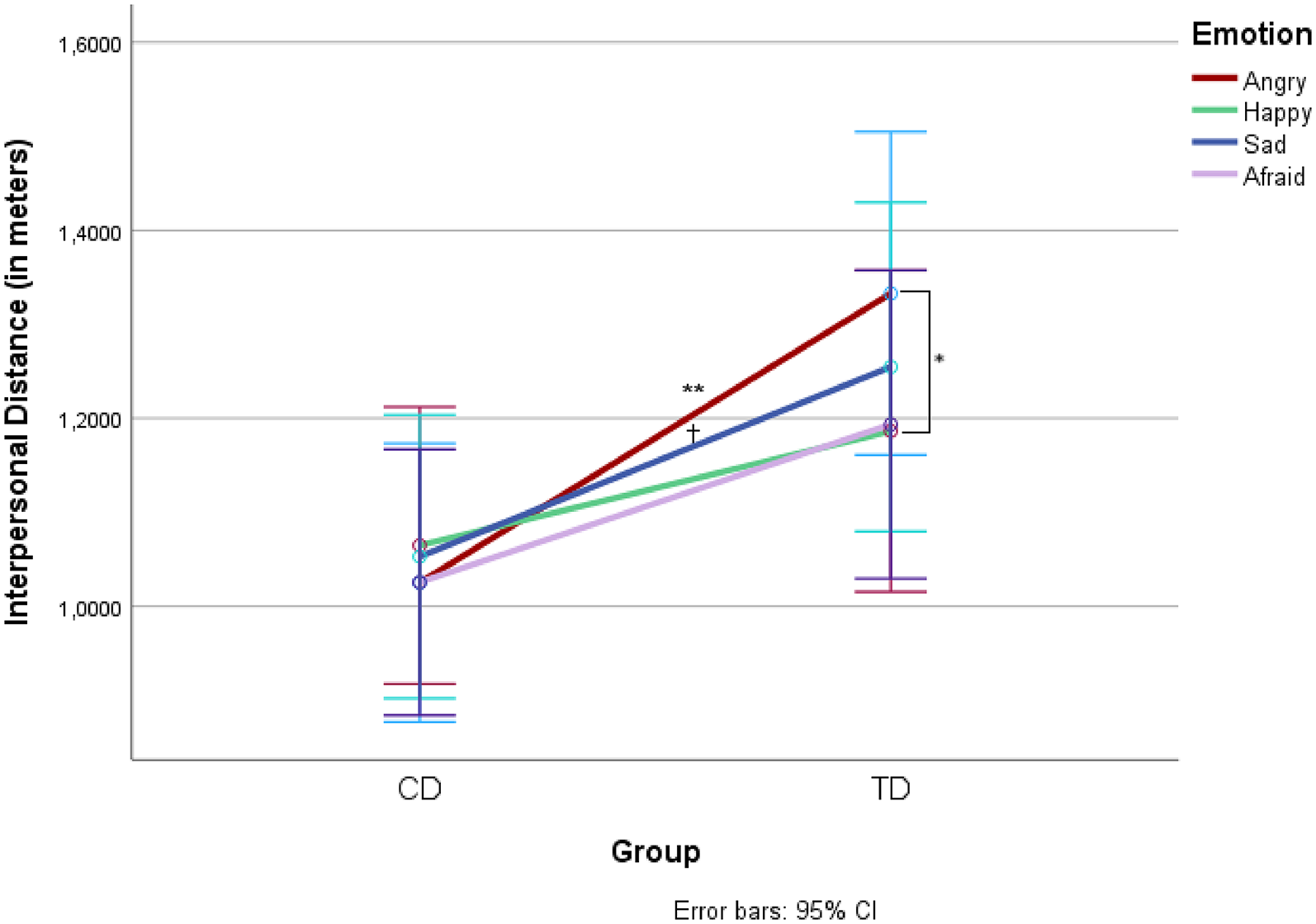
VR-data from indirect trials were investigated with two Repeated-Measures Analysis of Variance (rmANOVA) with Group (CD versus TD) as a between-subjects factor, Expression (Neutral, Angry, Happy, Anxious, Sad) as a within-subjects factor, and either WS or IPD as the dependent variable. VR-data from direct trials were investigated with a rmANOVA with Group (CD versus TD) as a between-subjects factor, Emotion (Angry, Happy, Anxious, Sad) as a within-subjects factor, and IPD as the dependent variable.
To better understand which facet of CU/SA contributed to significant associations with IPB and to control for individual differences in ER and the impact of COVID-19, 2-step hierarchical regression analyses across the whole sample were calculated. In these, ER and COVID-VAS-scores were included as predictors in the first step, either parent- or self-reported ICU and SASC total-scores in the second step, and those IPBs for which a significant group difference was found in the previous rmANOVAS were included as the dependent variables. This time, all participants, independent of their group were analysed together since CU-traits and SA are transdiagnostic phenomena that occur in the general population independently of psychopathology (e.g., [41]).
Because of the unequal group sizes (40 vs. 30), the resulting statistical power for the rmANOVAS was computed using a conservative estimate of the sample size (two groups of 30). For the critical mixed-factors 2 × 5 interaction on indirect trials, the power to find it significant was 1-ß > 0.99 for a large interaction effect, 1-ß > 0.99 for a medium-sized effect, and 1-ß = 0.46 for a small effect (all with p =.05 and r =.50). For the critical mixed-factors 2 × 4 interaction on direct trials, the power to find it significant was 1-ß > 0.99 for a large interaction effect, 1-ß > 0.99 for a medium-sized effect, and 1-ß = 0.42 for a small effect (all with p =.05 and r =.50). For the regression analyses, the power was 1-ß > 0.99 to detect large predictor effects (f2 = 0.35), 1-ß = 0.93 for medium-sized effects (f2 = 0.15), and 1-ß = 0.31 for small effects (f2 = 0.02).

留言 (0)