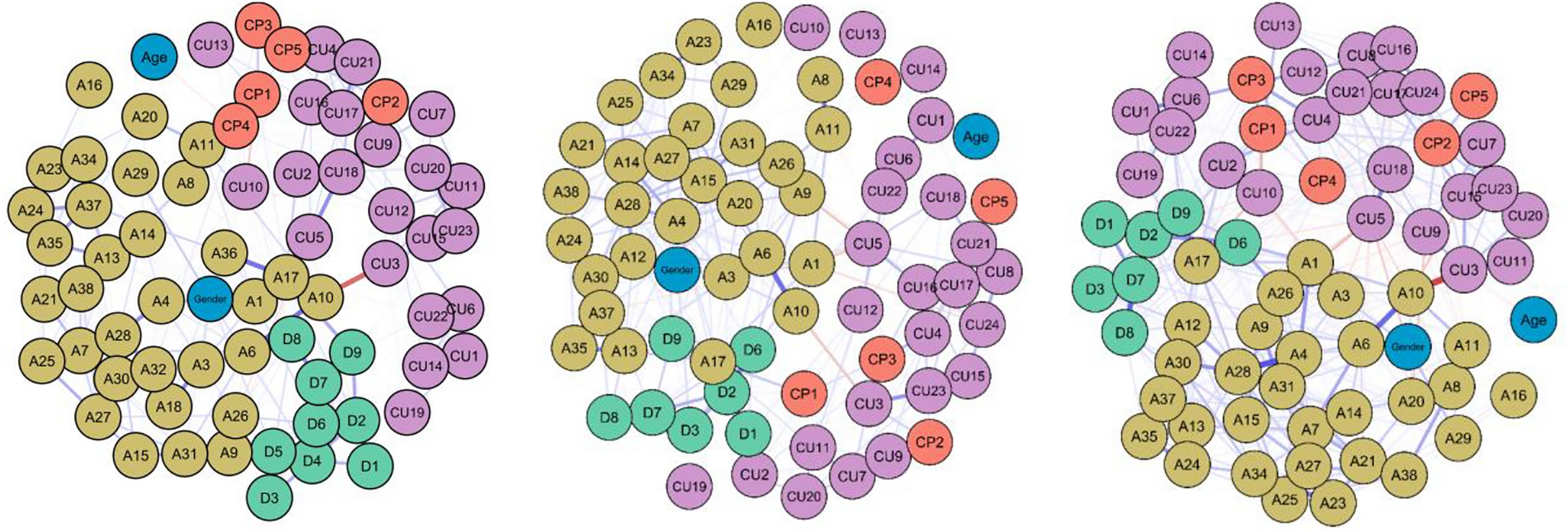
This cross-sectional study was conducted to assess the relationship between suicidal behaviour and various risk factors present in adolescents who have attempted suicide at least once. To facilitate interpretation of the results, only relationships whose absolute values were greater than or equal to 0.2 are taken into account [39].
Sociodemographic risk factors
Regarding age and sex, the quantity and intensity of the relationships established were lower than expected. Their positions are very peripheral, and correlations are scarce: age is not related to any other variable, and sex is related only to ADHD (male sex).
Contrary to the existing literature [48], there is no relationship between female sex and higher number of suicide attempts or greater intensity of suicidal ideation. Similarly, male sex did not exhibit greater lethality in suicide attempts. Regarding age, there was also no direct or inverse relationship with variables associated with suicide.
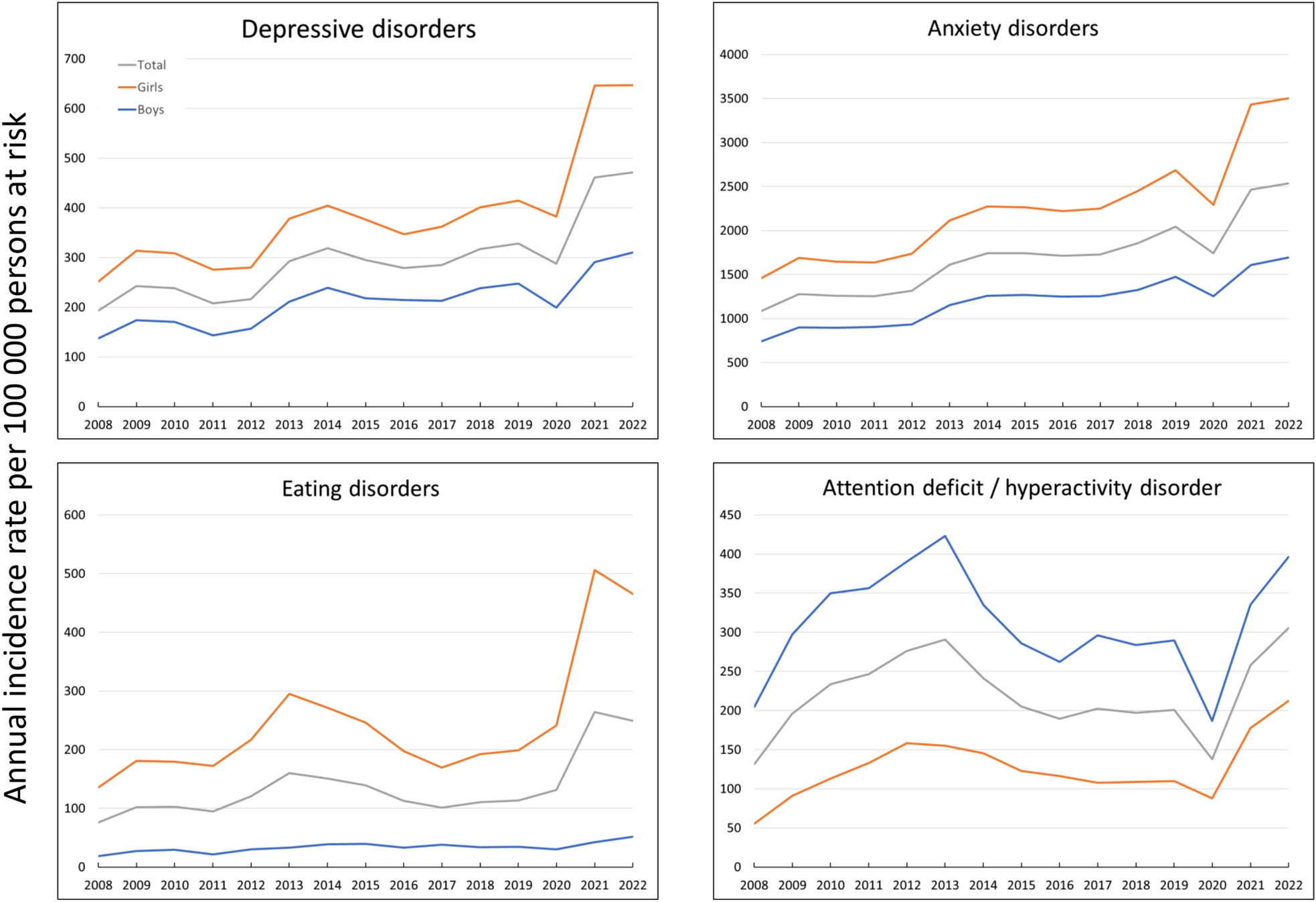
More recent studies and reviews have found that the influence of sex on suicidal behaviour in adolescents is age-dependent [49]. While there are sex differences in early and mid-adolescence, these differences tend to diminish as individuals grow older and become approximately equal by the age of 19 [50]. According to this study, the greatest differences between boys and girls regarding suicide attempts occur between the ages of 15 and 16. Given that the average age in our sample is 15, significant differences should be evident, but they are not observed. Several studies conducted among college students have been unable to establish significant sex-related differences, but the population in this case is older [49].
Our results may seem contradictory, but it is important to note that the majority of the sample consists of girls. It would be interesting to replicate the study in a sample with greater male representation to see if the expected differences in adolescence are revealed.
Migration
Migration appears to be a significant yet understudied risk factor for suicide [27]. Our findings indicate that, although it does not have a direct connection with suicide severity variables, it exhibits a more centralised distribution and is associated with trauma-related variables. Previous research indicates that mental well-being of migrants can be significantly impacted by pre-migratory circumstances, including traumas endured prior to and during the migration process [51].
Another noteworthy fact is the percentage of adolescents in the sample who have a history of migration. According to Spanish national statistics for the year 2022 [52], 10.2% of the population in Spain aged 12 to 17 years were born abroad, which is nearly half the percentage found in this sample. Despite the need for further in-depth analysis, this overrepresentation of migrants in our sample of suicide attempters highlights the vulnerability for suicide of this population.
Emotional and behavioural difficulties
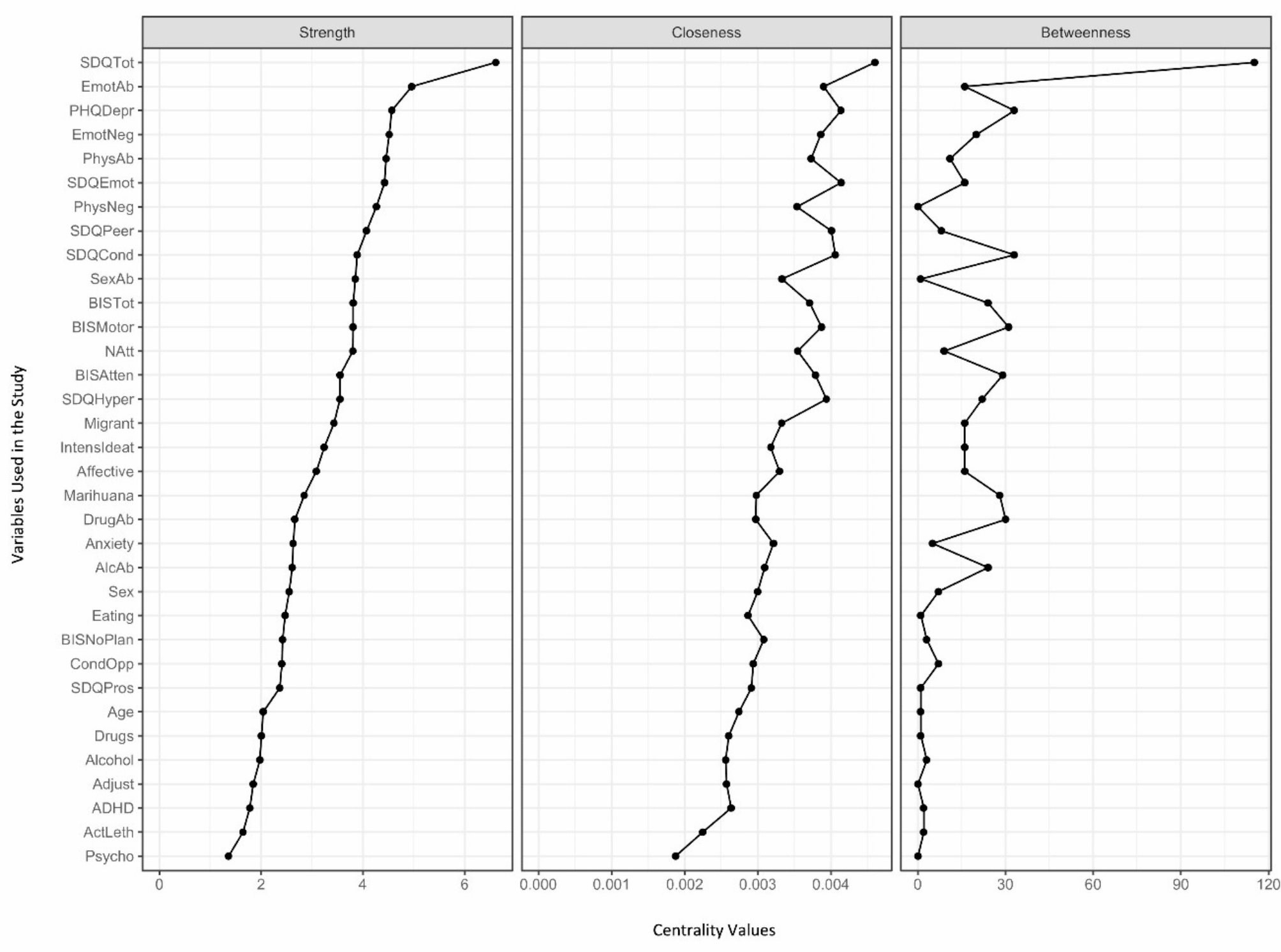
The SDQ variables exert the most significant influence on other variables and occupy central positions on the graph. Despite not being directly connected to suicide variables, the strong correlation between SDQ variables, especially emotional symptoms, and the PHQ-9 is of particular interest. This indirect association extends to the total number of suicide attempts.
The SDQ’s high closeness centrality signifies that it is more quickly reachable from other risk factors (i.e., through fewer steps) compared to other variables, functioning as a central hub in the network. This suggests that emotional and behavioural difficulties, as measured by the SDQ, act as key mediators or facilitators of other risk factors, enabling their influence to spread rapidly across the network. This central role underlines the SDQ’s critical importance within the overall structure of risk factors for suicidal behaviour.
Additionally, the SDQ’s high betweenness centrality indicates that it serves as a key connector or broker between other risk factors. Emotional and behavioural difficulties captured by the SDQ often mediate the relationships between other variables, playing an essential role in linking otherwise less connected factors. Therefore, the SDQ is significant not only for its direct impact but also for its ability to bridge various risk factors in the network.
The fact that the SDQ ranks highest across all three centrality measures (strength, closeness, and betweenness) underscores its pivotal role in the network of risk factors. Addressing the difficulties identified by the SDQ could potentially disrupt the broader risk factor network, thereby reducing the overall risk of suicide attempts. Interventions targeting these behavioural and emotional issues could have a significant ripple effect in mitigating suicide risk, given their central role in the network.
In the literature, there are few studies that link suicide to emotional and behavioural difficulties measured with the SDQ. There is one study conducted in 134 adolescents that focused on quality of life and suicide. It associates the SDQ emotional problems scale, SDQ peer problems scale, and SDQ total difficulties scale with a higher risk of suicide, especially in older adolescents [53]. Another study conducted in Korea found a relationship between the SDQ scale and increased suicidal behaviour in students, although it was based only on teacher’s reports [54].
On the other hand, the association between self-report measures and suicidality has been suggested in several studies, indicating that these questionnaires may be reliable and useful for evaluating suicide risk.
Regarding adolescents, specifically clinical population, studies indicate that self-report measures have been shown to be predictors of both suicidality and suicide attempts [55], not only in inpatients but also in Emergency Room [56].
The feasibility of using self-report measures in various settings, including schools and clinics, may make them advantageous for widespread screening. Their accessibility could contribute to an efficient assessment of suicide risk in diverse populations, facilitating timely interventions. Also, could empower adolescents to voice their experiences, fostering a supportive environment for discussing mental health issues.
The findings in the present study open a window of opportunities to study validated assessment quetionnaires in adolescents that may have significance when assessing suicide risk.
However, it’s important to recognize that such evaluations should not solely rely on diagnostic tools, as assessing suicide risk involves considering a broader range of factors.
Depression
In this study, depressive symptoms were assessed with both the PHQ-9 and the MINI-KID scale. The PHQ-9 shows stronger influence and centrality compared to the MINI-KID depression variable, establishing a greater relationship with SDQ variables, CTQ-SF variables, and total number of suicide attempts. Regarding the diagnosis of depression with the MINI-KID, despite being directly related to intensity of ideation, it occupies a more peripheral position on the graph and is less strongly associated with other variables. However, isolated links between anxiety disorders and alcohol abuse can be observed.
It is worth noting that the relationship between the PHQ-9 variable and depression assessed with the MINI-KID is very weak (and non-existent at a correlation threshold of 0.2), despite the fact that both measure similar items. No articles were found that compare or relate the PHQ questionnaire and the MINI-KID in assessing suicide risk or depressive symptoms in adolescents. Here we hypothesize about the possible causes of these findings.
On one hand, the PHQ-9 is a brief, self-administered questionnaire, which may make adolescents feel more comfortable reporting their symptoms. This accessibility can lead to greater honesty in their responses, potentially resulting in better detection of depression. Additionally, the PHQ-9 evaluates depressive symptoms within a two-week timeframe, which may be more relevant for some adolescents who might not recognize or recall more chronic depressive symptoms that the MINI-KID aims to identify. It is also important to consider that the patients have recently attempted suicide and are experiencing a higher level of distress in the previous days.
Furthermore, the validity of each tool may vary depending on the specific population being assessed. In this case, the study sample includes a higher proportion of female adolescents, who are generally more likely to recognize and express their emotions [57]. This may explain why the PHQ-9 could more accurately reflect their subjective experiences.
Finally, the conditions under which the questionnaire are administered, as well as the relationship between the evaluator and the evaluated, can influence the results. If adolescents feel more comfortable with the approach of the PHQ-9, this may translate into more accurate responses.
A Spanish literature review identified psychological factors (depression, anxiety, previous suicide attempts, drug and alcohol use, and other comorbid psychiatric disorders), life stressors (family problems and peer conflicts), and personality traits (neuroticism and impulsivity) as factors that can increase the risk of suicidal behaviour [25]. Supporting the multifactorial origin of suicidal behaviour, a study comparing suicidal behaviour in adolescent Swedish twins found that suicide attempts were related to childhood psychopathology in a general sense, as well as genetic factors. However, when studying specific individual factors such as inattention, opposition, and anxiety, no statistically significant relationship was found with suicide attempts or self-injurious behaviours [17].
Based on our results, this study aligns with some of those previously discussed the literature, in which depression emerges as one of the most significant risk factors [8, 9]. Furthermore, when assessing depressive symptoms in patients with a recent suicide attempt, it may be advisable to use the PHQ-9 questionnaire rather than the MINI-KID.
Childhood trauma
As expected, all the subscales of the CTQ-SF have a centralised position, closely related to SDQ variables, PHQ-9, and migrant situation and are also closely related to each other. Subscales for emotional abuse, sexual abuse, and physical abuse also are strongly associated with the number of previous suicide attempts.
A review of studies that relate suicide to different types of reported trauma found that extensive literature exists. In a study conducted in Brazil with a cohort of over a thousand young individuals, a decreasing magnitude of risk was observed for emotional abuse, emotional neglect, sexual abuse, physical abuse, and physical neglect [58]. In European [59] and clinical populations, a higher risk was found for emotional abuse than the other types of trauma [60, 61].
In this cohort, patients with a history of migration are most closely associated with physical abuse and neglect, followed by emotional abuse and neglect. As previously discussed, these forms of abuse are the least closely related to suicide. However, it would still be advisable to assess traumatic history in migrant patients.
Impulsivity
In this case, the data aligns with the controversial existing literature. On one hand, the placement of BIS-11 variables on the graph is more peripheral compared with trauma-related variables, PHQ-9 or SDQ, indicating their lesser influence. Specifically, only the BIS-11 motor subscale shows close direct relationships with different SDQ variables. No relationship was found with variables related to suicide attempts or variables associated with depression. However, the BIS-11 attentional subscale shows an inverse relationship between the SDQ and emotional neglect.
Based on the findings presented here, we deduce that the influence of impulsivity on suicide is not direct, however, it could potentially have an indirect influence through other variables such as the SDQ. It is important to note that BIS motor impulsiveness appears to exert the most influence, which aligns with the reviewed literature [14]. This may be due to several reasons. Motor impulsiveness involves acting on impulse without deliberation, which can lead to spontaneous and potentially dangerous behaviors, including self-harm and suicide attempts. Also when individuals experience intense emotional distress, those with high motor impulsivity may be more likely to engage in suicidal actions as a means of coping or escape.
Drug consumption
Based on the presented graphs, the pathology related to alcohol and drug use does not show any relationship to variables associated with suicide attempts. Similarly, consumption of alcohol or drugs prior to the attempt does not appear to be related to the study variables.
As expected, substance use is related to itself, and alcohol-related pathology is associated with affective disorders (MINI-KID). Regarding centrality measures, all variables are situated at the bottom of the graph.
Based on our results, we conclude that the influence of substances in this case is minimal. Although some studies report the contrary [16, 18, 19], our results support the findings of some of the reviewed articles. For example, a large-scale American study conducted with a cohort of over 18,000 patients found that having an alcohol use disorder is a risk factor for young adults but not for adolescents. Additionally, they did not find any association between pathology related to the use of other substances and suicide, regardless of age [20]. One possible reason is that adolescents tend to consume alcohol and other substances in a more sporadic and experimental way. As a result, the secondary problems related to substance use may be more severe and frequent with long-term chronic use. Additionally, it is possible that the detection and diagnosis of substance use are underestimated, as the information is collected through interviews, which might reduce the honesty of responses, even without parents present. Finally, when interpreting these results, it is important to consider that the proportion of patients with a clinical diagnosis is small. As previously mentioned, the patients may still be too young to have developed full-blown substance-related pathology. In the future, it could be more valuable to collect information about consumption patterns, rather than focusing solely on established pathology.
Influence on severity of suicidal behaviour
In relation to variables associated with severity of suicidal behaviour, the variable that shows the strongest relationships with others and has a more central position is the number of attempts variable. On the other hand, lethality of attempt is the least influential variable, as it does not show associations with any other variables beyond a correlation above 0.2. Another noteworthy finding is that the variables studied do not exhibit significant relationships with each other.
This association may have particular relevance in clinical practice for assessing the risk of suicide in patients who have already made a previous attempt. According to the results we obtained, higher scores on the SDQ scale (especially total scores) and higher scores on the PHQ-9 scale may be associated with a higher risk of reattempting, as they are correlated with a greater number of previous attempts. It is important to consider this when choosing a diagnostic support scale.
Strengths and limitations
The results of this study must be interpreted in the context of certain limitations. First, the cross-sectional design of the study makes it difficult to to establish the direction of the findings. On the other hand, although the sample includes many patients from a clinical perspective, from a statistical point of view, it would be desirable to obtain a larger sample to achieve greater power. Another limitation is that the distribution by sex is very unbalanced, with very few patients identified as male. This, combined with the fact that it is a clinical population, could limit the extrapolation of the results to the general adolescent population. Another limitation to consider is the use of a version of the MINI-KID whose diagnostic criteria are based on the DSM-IV-TR. This makes the values outdated and complicates comparison with future research. Finally, another factor that complicates this comparison is the lack of studies conducted with the same methodology.
Despite the limitations described above, the study has several strengths to consider. One of the greatest strengths of the study is having a sample of patients in an understudied population, such as adolescent patients, using an innovative approach to the well-studied risk factors for suicide. Although the population under study is very specific, a relatively large sample has been achieved. This has been possible due to the collaboration among multiple centers across Spain. In addition to increasing the total sample size, this collaboration enhances its representativeness.
Another strength of the study is the methodology used to assess the adolescents. The evaluators were professionals with extensive experience in the field, and validated assessment instruments have been used, combining self-administered questionnaires with those administered by the evaluator. In addition, the assessment space provided confidentiality to create a trusting environment for the patient.

留言 (0)