
記住我


The current study was conducted after obtaining approval from the Research Ethics Committee of the Faculty of Dentistry at Minia University, Egypt (Committee No. 103, registration No. 893, date: 30/1/2024).
Sample size calculationA power analysis was conducted to ensure adequate power for applying a two-sided statistical test of the null hypothesis, which posits that no difference exists between the tested groups regarding measured fracture resistance. By adopting an alpha (α) level of 0.05, a beta (β) level of 0.2 (power = 80%), and effect size (d) of 1.10, calculated based on the results of a pilot study involving ten samples in each group, the total required sample size (n) was determined to be 30 samples (15 samples per group). Sample size calculation was performed using R statistical analysis software, version 4.3.2 for Windows (Vienna, Austria).
Sample selection (strict criteria were applied for the selection of the teeth)A total of 30 freshly and atraumatically extracted human intact mature maxillary second premolars, possessing Vertucci’s type I root canal configuration [21] and nearly straight roots with an equivalent curvature angle of less than 10º as determined by Schneider’s method [22], were collected from the outpatient clinic at the Faculty of Dentistry, Minia University, Egypt after obtaining the respective patient’s informed consent. Anatomical matching for the selected teeth and their pulp morphologies and volumes was achieved using 3D imaging (Papaya 3D plus, Genoray, Gyeonggi-do, Korea). Tooth dimensions were measured using a digital calliper with an accuracy of 0.01 mm. The buccolingual dimension of the selected teeth was 9.5 ± 0.5 mm, while the mesiodistal dimension was 7.5 ± 0.5 mm. To standardize the tooth length for all samples, occlusal reduction was performed, setting the tooth length at 21 mm from the buccal cusp tip as a reference point. Teeth presenting coronal or root caries, calcified canals, pre-existing root canal fillings, teeth extracted more than 1 month before conducting the experiments, and external or internal resorptive lesions were excluded. Additionally, teeth were inspected for evidence of cracks or fractures using a dental operating microscope (DOM) (Magna Labomed, Labo America Inc., 920 Auburn Court Fremont, CA 94538, USA) at a magnification of 20X. Subsequently, the teeth were cleaned from any hard or soft tissue deposits, disinfected for 30 min in a 5.25% sodium hypochlorite solution (NaOCl) (Omez, Phar Omez, Pharaonic Pharmaceuticals, Egypt), and finally immersed in a 0.1% thymol solution (Formula e Acao, São Paulo, SP, Brazil) for the same period until use [23].
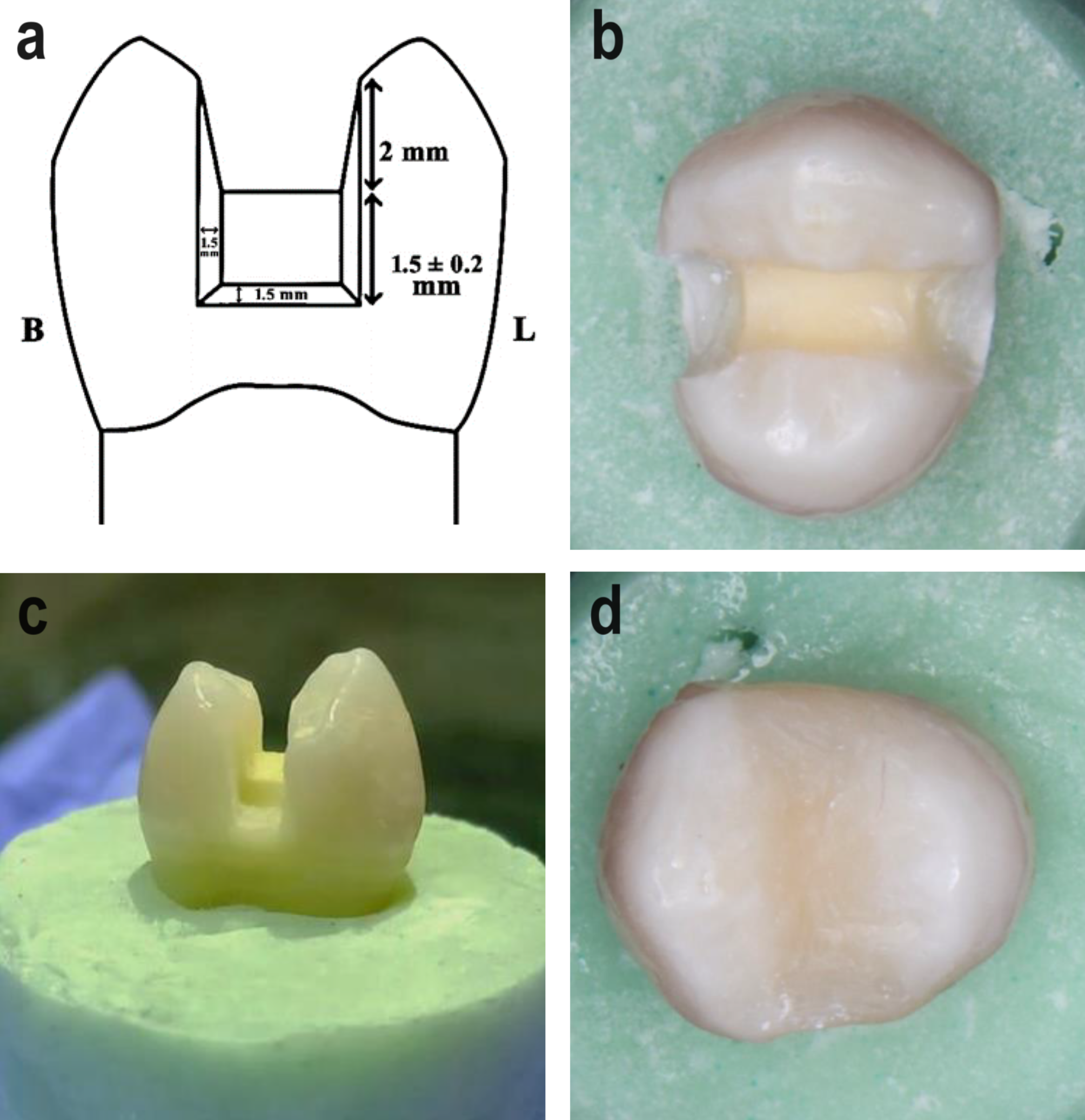
Teeth mountingTwo half-split Teflon moulds, each measuring 25 mm in height and 30 mm in diameter, were utilized. After pouring self-curing resin into the mould, each tooth, with a stretch film surrounding its root, was submerged in acrylic resin up to 2 mm apical to the cementoenamel junction (CEJ) to simulate the bone level. A Dental Surveyor (Ney Dental Surveyor, Anaheim, CA, USA) was employed to position each tooth inside an acrylic block, ensuring proper centering and alignment parallel to the tooth’s long axis. The teeth with the stretch film were taken out once the acrylic resin had hardened and reinserted after a light body silicone (Elite HD; Zhermack SpA, Badia Polesine, Italy) was injected into the root cavity to mimic the periodontal ligament. Any extra impression material was removed using a #12 scalpel. Mesio-occluso-distal (MOD) cavities were prepared using a carbide bur (straight round end fissure #245; Kerr, Kloten, Switzerland) operated in a high-speed handpiece (Sirona, Erlangen, Germany) with water cooling. The occlusal isthmus width was set at one-third of the intercuspal distance, with measurements of 2 ± 0.2 mm pulpal depth, 1.5 ± 0.2 mm axial height, 1.5 ± 0.2 mm axial depth, and 1.5 ± 0.2 mm gingival width (Fig. 1a-c) [24].
Fig. 1
Cavity preparation and initial restorative procedures: (a) scheme showing the dimensions of the prepared cavity; (b) occlusal view; (c) proximal view, (d) MOD composite resin initial restoration
Restorative proceduresAll restorative procedures were carried out by a single specialist with 23 years of experience in Restorative Dentistry (N.E.M.). The enamel cavity walls of each prepared premolar were etched using 37% phosphoric acid etching gel (Total etch, Ivoclar Vivadent, Zurich, Switzerland), applied for 15 s, rinsed with water for an additional 15 s, and gently air-dried. Per the manufacturer’s instructions, after evenly applying the bonding agent (Adhese universal, Ivoclar Vivadent) to the cavity walls, the material was rubbed for 20 s with a micro brush (3MTM XS Applicator Brushes; 3 M St. Paul, MN, USA), then gently dried with oil-free air to remove any remaining solvents. Subsequently, the material was light-cured for 20 s using a light-emitting diode curing unit (3 M Elipar Deep Cure-S LED Curing Light; 3 M St. Paul, MN, USA) with a light intensity of 1470 mW/cm². Each tooth was encircled by a Tofflemire matrix system (Medicaline, Bunkyo-ku, Japan) before composite packing, and a gold-plated composite applicator (American Eagle composite set, West Chester Township, Ohio, United States) was utilized to pack the resin composite restorative material A3 (Tetric N-Ceram, Ivoclar Vivadent, Zurich, Switzerland) incrementally into each prepared cavity using the oblique layering technique in order to reduce the c-factor and prevent distortion of the cavity walls [25,26,27,28]. Following the manufacturer’s instructions, each increment was light-cured for 20 s. To achieve the proper mesiodistal and occlusal contour, as well as the ridges and inclines of the occlusal anatomy, the last 2 mm increment was placed occlusally to over-fill the cavity, then light-cured for 20 s. Finishing and polishing were conducted using the TOR VM Finishing and Polishing Kit (TOR VM, Moscow, Russia) (Fig. 1d).
Aging procedures (thermo-mechanical cycling fatigue)A four-station multi-modal ROBOTA chewing simulator (ACTA Fatigue tester, Amsterdam, Netherlands) with servomotor control (Model Ach-09075dc-T, Ad-Tech Technology, Berlin, Germany) and a thermo-cyclic protocol was employed to conduct the mechanical aging test. Using ROBOTA, simultaneous motions in both vertical and horizontal directions under thermodynamic conditions were simulated. Each chamber consists of an upper, hardened steel stylus holder that can be securely screwed tight to serve as an antagonistic material and a lower plastic sample holder where the specimen can be embedded. Five kilograms of weight, equivalent to 49 N of chewing force, were applied. The following settings were employed for the chewing simulation: a cycle frequency of 1.6 Hz, rising/forward speed of 90 mm/s, descending/backward speed of 40 mm/s, horizontal movement of 1 mm, and rising/vertical movement of 3 mm. The specimens underwent 75,000 cycles with 6000 thermal cycles (5˚/55˚C, dwell period of 25 s) to replicate six months of intraoral aging [29].
Specimen groupingTeeth were numbered and randomly allocated into two groups based on whether the coronal restoration was entirely or partially replaced: the totally replaced restoration (TR) group (n = 15) involved the preparation of a traditional access cavity after the complete removal of the pre-existing coronal restoration, while the partially replaced restoration (PR) group (n = 15) involved accessing the tooth through the pre-existing restoration without the need for its complete removal. All endodontic and subsequent restorative procedures were performed by a single endodontist with 20 years of experience in endodontics (M.T.).
TR group: After completely removing the pre-existing coronal restoration, a traditional access cavity was prepared following common guidelines for access cavity preparation, aiming to establish straight-line access to canal orifices with smoothly divergent cavity walls [30, 31]. This design was achieved using a round diamond bur #801 − 014 (Komet, Brasseler, Lemgo, Germany) to remove the entire roof of the pulp chamber. Subsequently, the cavity walls were refined using a tapered carbide fissure bur (Komet H33L, Komet Brasseler). All access cavity burs were mounted on a high-speed handpiece with water spray. The access cavities were prepared while maintaining the following wall thicknesses, as outlined in an earlier study by Garlapati et al. [32]: the buccal wall measured 2 mm at the occlusal surface and 2.5 mm at the gingival floor level, and the palatal wall measured 1.5 mm at both gingival floor level and occlusal surface. The widths of the remaining wall thickness were measured using a digital calliper (Fig. 2a).
Fig. 2
Gaining endodontics access: (a) totally replaced restoration access; (b) partially replaced restoration access; (c) illustration of the post-endodontic restoration
PR group: Under a magnification of 16X using a dental operating microscope (DOM), an access cavity was prepared through the pre-existing restoration using a diamond round bur # 806 − 010 (Komet, Brasseler), mounted on a high-speed handpiece with water spray, with maximal preservation of the remaining restoration and tooth structure. The access opening was standardized in all samples, leaving 0.5 mm of the restoration buccally and palatally, while 2.5 mm of the restoration was left mesial and distal to the access cavity (Fig. 2b).
Root canal preparation and fillingRoot canal preparation and filling procedures were similar for both groups. After access cavity preparation, patency was verified using a manual stainless-steel K-file ISO size 10 (Dentsply, Maillefer, Ballaigues, Switzerland). Any teeth failing to demonstrate patency were excluded from the study. Working length was visually determined by inserting a stainless-steel K-file ISO size 10 into the root canal until it became visible through the apical foramen, then subtracting 1 mm from this measurement. All teeth were instrumented up to size 40/0.04 (Hyflex CM, Coltene Whaledent, Cuyahoga Falls, OH, USA) and received identical volumes of irrigation according to the standard protocol, which involved using 2 ml of 5.25% NaOCl solution for 20 s between files, followed by a final rinse alternating between 10 ml of 5.25% NaOCl solution for 2 min and 10 ml of 17% ethylenediaminetetraacetic acid (EDTA) solution for 2 min, with an intermediate rinse using the same volumes of saline solution [33, 34]. A final flush with saline solution was performed to eliminate any remaining irrigant residues [35]. After root canal preparation was completed, the canals were dried using size 40/0.04 paper points (Coltene Whaledent) and obturated using a single-cone technique with a matched master gutta-percha cone size 40/0.04 (Coltene Whaledent) and a bioceramic sealer (EndoSequence BC sealer, Brasseler Blvd, Savannah, USA). The coronal end of the root canal filling was standardized to be 1 mm below the canal orifices. The pulp chamber was cleaned using a cotton pellet soaked in 70% alcohol to remove any sealer residues. The quality of obturation was assessed using conventional periapical radiographs.
Final coronal restorationTR group: Upon completion of endodontic procedures, the access cavity was sealed with a new resin composite restoration. This involved etching the cavity enamel surfaces, applying adhesive to all cavity walls, and using bulk-fill flowable resin composite (Tetric N-Flow Bulk Fill, Ivoclar Vivadent, Zurich, Switzerland ) according to the manufacturer’s instructions to fill most of the cavity, leaving only 2 mm for the final resin composite filling (Tetric N-Ceram, Ivoclar Vivadent, Zurich, Switzerland). The restoration was then packed, cured, finished, and polished as previously described (Fig. 2c).
PR group: Acid etching and bonding application were carried out as previously described for the surfaces of the access cavity and old composite restoration. Bulk-fill flowable resin composite (Tetric N-Flow Bulk Fill, Ivoclar Vivadent, Zurich, Switzerland ) was applied to fill most of the access cavity and light-cured for 20 s, leaving only 2 mm for the final resin composite filling (Tetric N-Ceram, Ivoclar Vivadent, Zurich, Switzerland ). This was followed by light curing for 20 s, finishing, and polishing (Fig. 2c).
Final aging procedures (thermo-mechanical cycling fatigue)The final coronal restoration was aged using the Robota chewing simulator for an additional 75,000 cycles with 6000 thermal cycles (5˚/55˚C, dwell period of 25 s), equivalent to six months of intraoral aging.
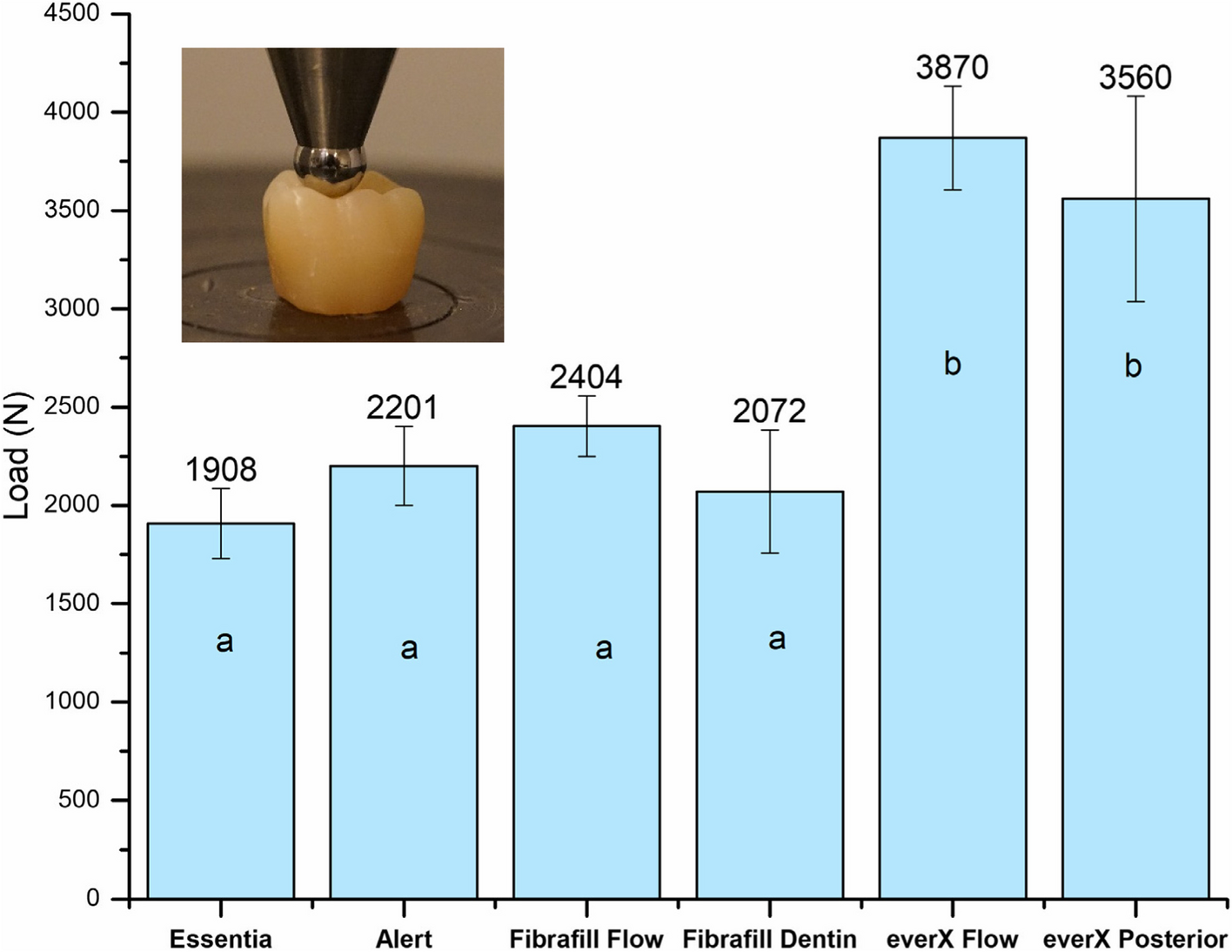
Measurement of fracture resistance (static fracture test)All samples were individually mounted on a computer-controlled materials testing machine (Model 3345; Instron Industrial Products, Norwood, MA, USA) equipped with a load cell of 5 kN, and data were recorded using computer software (Bluehill Lite Software, Instron®). The samples were secured to the lower fixed compartment of the testing machine by tightening screws. The fracture test was conducted by applying compressive load occlusally in a direction parallel to the long axis of the root using a metallic rod with a round tip (2.6 mm diameter) attached to the upper movable compartment of the testing machine, which travelled at a cross-head speed of 1 mm/min. The load at failure was indicated by an audible crack and confirmed by a sharp drop in the load-deflection curve recorded using computer software (Bluehill Lite Software, Instron® Instruments). The load required to cause fracture was recorded in Newton.
Failure mode assessmentFailure modes were examined by an independent evaluator who was blinded to the experimental procedures using a USB digital microscope (U500x Digital Microscope, Guangdong, China) at a magnification of 35X. Images were captured and transferred to a personal computer equipped with image analysis software (Image J 1.43U, National Institute of Health, USA) to determine the failure mode pattern, whether it was a repairable fracture (where the restoration’s fracture would occur above the CEJ) or an irreparable fracture (where the fracture of the coronal restoration would occur below the CEJ) [36].
The images were captured using the following image acquisition system: a digital camera (U500x Digital Microscope, Guangdong, China) with 3 megapixels of resolution, positioned vertically at a distance of 2.5 cm from the samples; the angle between the axis of the lens and the sources of illumination was approximately 90°; plus illumination was provided by 8 LED lamps (adjustable by the control wheel), with a colour index close to 95%. The images were captured at maximum resolution and connected to a compatible personal computer using a fixed magnification of 35X. Each image was recorded with a resolution of 1280 × 1024 pixels.
Statistical analysisThe Shapiro-Wilk test was used to assess the assumption of normality of the fracture resistance test outcomes. Considering the Gaussian distribution of the outcomes, the groups with totally or partially replaced restorations, whose results were expressed in means and standard deviations, were compared using the Independent Samples t-test. Regarding the results of failure modes, the Chi-square test was used to compare the types of failure modes across the analyzed groups. The significance level was set at 5% (SPSS v22.0 for Windows; SPSS Inc., IBM, Zurich, Switzerland).
留言 (0)