
記住我






This study systematically evaluated the incidence and characteristics of maxillary lateral incisor dens invaginatus in China on CBCT images according to Oehlers’ classification and Gu’s classification, and analyzed the impact of radicular invaginatus on periodontal supporting tissues preliminarily.
The diagnosis and classification criteria for dens invaginatus are constantly updated, and the reported incidence varies greatly due to the choice of diagnostic techniques and race. In terms of diagnosis and classification criteria, this study selected Oehlers' classification criteria to determine coronal invaginatus, which has been widely accepted [7]. The radicular dens invaginatus is categorized into two main types: radicular cystoid invaginatus [8] and radicular groove, with the severity of radicular groove assessed using the Gu’ classification [9]. The Gu’s classification is relatively clear and closely related to clinical prognosis.
In terms of diagnostic techniques, previous studies have used imaging methods such as periapical films, panoramic radiographs, and CBCT to identify dens invaginatus. In clinical practice, periapical films are the most commonly used diagnostic method, but they are prone to misdiagnosis for dens invaginatus [25]. Capar et al. reported that CBCT could significantly improve the detection rate of dens invaginatus. By observing the rendered panoramic images of 300 Turkish patients, the detection rate of tooth invagination was 3%, while three-dimensional observation could improve this detection rate to 10.7% [26]. Thus, this study chose CBCT images to identify dens invaginatus.
As shown in Table 1, the incidence of coronal invaginatus is 12.3% and the incidence of radicular invaginatus is 14.6%. For a more comprehensive evaluation, we also calculated the incidence of coronal or radicular invaginatus in maxillary lateral incisors, with a value of 25.0%. In 2023, a meta-analysis summarized the incidence of coronal invaginatus in anterior teeth using CBCT, ranging from 1.1% to 13.5%, with the maxillary lateral incisors being the most affected teeth [11]. In our study, the incidence of coronal invaginatus was 12.3% (26/212). The relatively high incidence may be due to smaller voxel size (0.3 mm) and smaller slice thickness (0.3 mm) during CBCT acquirement. As for the incidence of radicular invaginatus, there are very few related articles, especially those that refer to the Gu’s classification. The limited data reported the incidence of 2.3%—7.3% [3, 13,14,15]. However, all the relative subjects were Caucasian. In our study, the subjects were Mongolian, and the incidence of radicular invaginatus is 14.6% (31/212). Our findings suggested that, besides the impact of different CBCT setting parameters, radicular invaginatus may occur more frequently in Mongolian.
In this study, no cases of radicular cystoid invaginatus in the enlarged root were observed. All of 31 radicular dens invaginatus exhibited radicular grooves. More than 90% (90.3%) of the radicular grooves occurred at the mesial or distal palatal sites, and nearly 90% (87.1%) of the radicular grooves ended within the coronal third of the root (Fig. 3). It is worth noting that one tooth of Gu’s type III was present, with an additional root (Fig. 2B). A root furcation was observed between the additional root and the main root. Once this furcation involvement became three or four degrees, the prognosis of this dens invaginatus tooth may be poor, just like posterior teeth with penetrating furcation involvement. This article is followed by a case of combined endo-periodontal disease of a maxillary lateral incisor with an additional root. Interestingly, through sequential treatment, the separation of periodontal and periapical lesions was achieved, which may obtain more autologous bone regeneration and more definite periodontal new attachment (Fig. 4).
Fig. 4
Endo-periodontal therapy of a Gu’s type III tooth with an additional root. A, fistula presentation after initial therapy; B, palatal gingiva was dark red; C, an additional root; D, the depth of infrabony pocket was 8 mm; E, additional root resection; F, endodontic filling; G, the additional root was 9 mm in length with root canal; H, 5 months after resection, the fistula disappeared; I, PD was 8 mm at the palatal site; J, the depth of mesial infrabony defect was 5 mm; K, new bone was obtained after root resection in the mid-root; L; the depth of palatal infrabony defect was 3 mm; M, bone graft and membrane overlay. N, suture after periodontal regeneration surgery; O, 9 months after regeneration, mesial PD was 5 mm; P; palatal PD was 3 mm; Q, the original infrabony defect was filled with new alveolar bone; R, apicectomy; S; suture after apicectomy; T, 8 months after the completion of endo-periodontal therapy, PD was 3 mm in the mesial; U, PD was 2 mm in the palatal; V, periapical film (V1) and CBCT (V2) of tooth 22 at first visit; W, radiological examination, periapical film (W1) and CBCT (W2), at 5 months after additional root resection; X, periapical film immediately after periodontal regeneration surgery; Y, periapical film before apicectomy; Z, 8 months after completion of endo-periodontal surgery. Yellow arrows show substantial bone generation after root resection
Previous reports on dens invaginatus were mostly single or several case reports. That is, using a variety of combined treatment methods, such as root canal therapy, root resection, root surface treatment, bone graft, guided tissue regeneration and even intentional replantation, to control infection and increase the attachment of periodontal support tissue as much as possible. For invaginatus deep to the apex, there were also reports of extraction [27,28,29,30,31,32,33].
The above case reports showed that clinicians have already realized that the invaginatus site is an area where bacteria are easy to stay and difficult to be controlled, and oral pathogenic bacteria could destroy the tooth and periodontal tissue through this access quickly, leading to caries, pulpitis, periapical lesion and periodontal support tissue loss. In 2021, Tan et al. obtained the microbiota from the radicular groove of four replanted teeth and sequenced it. The results showed that the bacterial communities at this site had dual characteristics of pulp and periodontal infections, suggesting that the radicular groove may be a bacteria bank and play an interaction bridge between the root apex and tooth cervix [34]. For endodontic treatment, there may be small hidden channels between the invaginatus area and the pulp tissue, often accompanied by complex root canal system morphology, which brings great challenges to infection control and reduces the prognosis of root canal therapy seriously. For periodontal prognosis, the root surface groove naturally lacks normal periodontal attachment. As a result, even after root surface treatment and filling of various types of biomaterials, it is difficult to form effective new attachment after regenerative surgery at the radicular groove surface, worsening the periodontal prognosis.
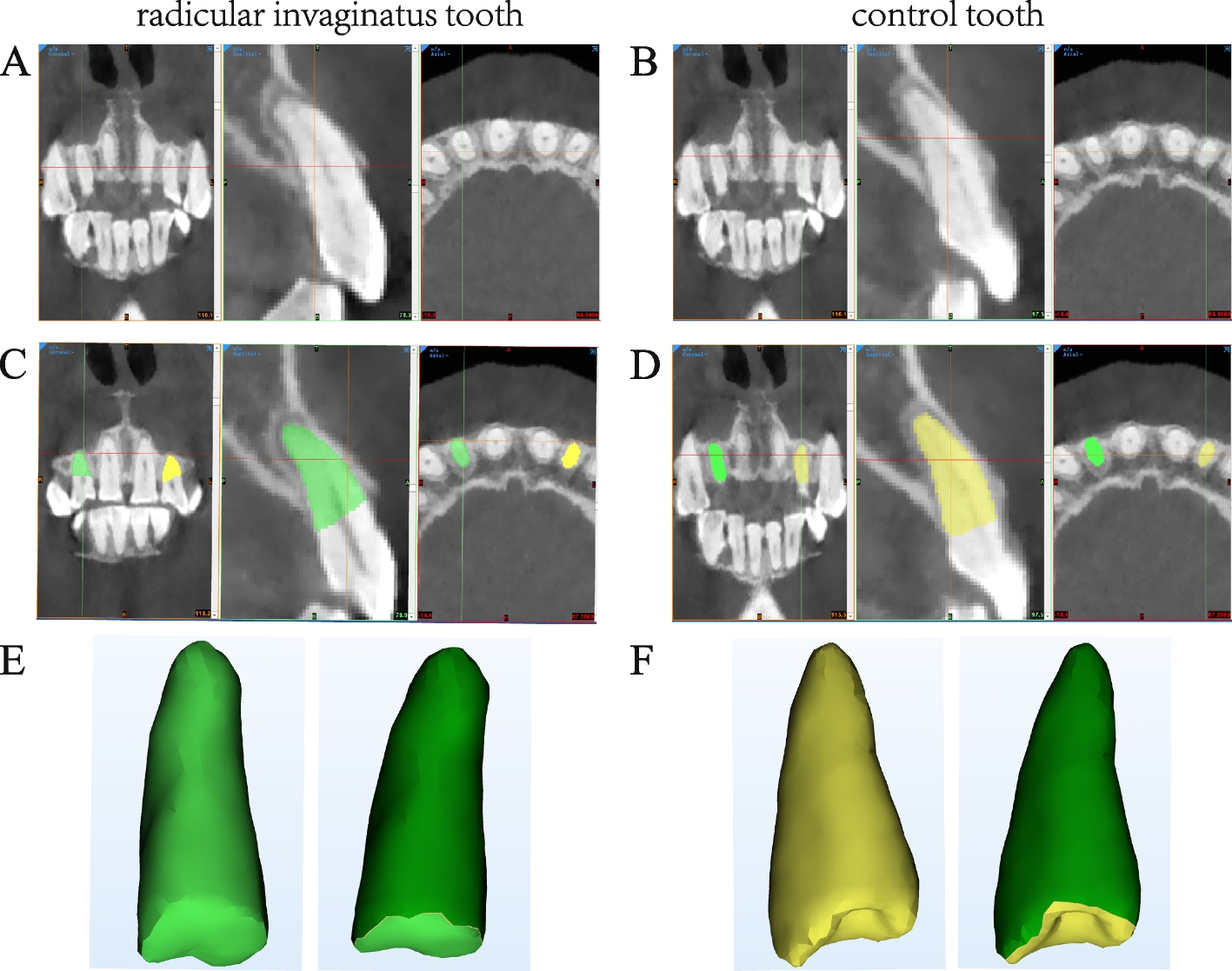
However, so far, only few studies reported the impact of radicular invaginatus on periodontal tissues. Limited results showed that the infection index, such as gingival index, plaque index, and bleeding index at the groove site were more severe than control sites [20, 21]. Periodontal ligament area is the key to periodontal prognosis. This study attempted to analyze whether radicular invaginatus is accompanied by a reduction of the periodontal ligament area using a split-mouth control method. The results show that the periodontal ligament area of the maxillary lateral incisor with radicular invaginatus is smaller than that of the control tooth of the same name on the same jaw (148.93 ± 35.62mm2 Vs. 152.28 ± 40.22mm2). Although this difference may not be statistically significant due to the small sample size, the results provide a quantitative analysis of the periodontal ligament area of the affected and control teeth, providing a theoretical basis for the phenomenon of radicular invaginatus accompanied by a reduction in periodontal support tissues.
留言 (0)