
記住我







Cancer is the second leading cause of death globally, and according to estimates from the World Health Organization (WHO, 2019) in 112 countries, it is either the first or second most common cause of death1. With the increase in life expectancy, the burden of cancer in elderly adults is also increasing, and higher incidence and mortality are seen among them as compared to younger ones2,3. Earlier estimates of GLOBOCAN 2012 showed that worldwide a total of 6.7 million older persons (≥65 yr) were diagnosed with cancer, accounting for 47.5 per cent of all cases, and of all elderly burden, 48 per cent occurred in less developed regions4. Another global study projected that compared to 2018, a 200 per cent increase in cases could be seen for those aged ≥80 yr by 20505.
With the world population ageing, it is projected that by 2030, 1 in every 6 persons globally will be aged ≥60 yr and by 2050, the two-thirds population in lower-middle-income countries (LMICs) will be elderly6,7. This will lead to an increase in both numbers of new cancer cases and deaths. The increasing burden will make the role of geriatric oncology immense in the coming years to ensure the functional, nutritional, cognitive, and psychosocial functioning of elderly cancer patients.
An in-depth, recent knowledge of the variation of the global cancer pattern among older populations by world regions, cancer sites or gender will provide significant current information to health planners and policymakers in developing global geriatric cancer control policies. This study was conducted to find out cancer incidence and mortality patterns among older adults aged 60 yr or above in different continents.
Materials & MethodsCancer incidence and mortality with future estimates were estimated from the data obtained from the publicly available Global Cancer Observatory - GLOBOCAN 2020 online database (gco.iarc.fr-cancer today, cancer tomorrow and cancer over time). The International Agency for Research on Cancer (IARC) includes data for all cancer sites (ICD-10, C00-C97, except C44) combined, available for 185 countries or territories for 36 different types of cancer by sex and age group8-10. For continent-wise analysis, data were extracted and reported for Asia, Europe, Northern America, Africa, Latin America and Caribbean, and Oceania (as per IARC-WHO methodology to report cancer statistics based on United Nations Population Division ( https://gco.iarc.fr/today/en/data-sources-methods )8-10. The study was conducted at the ICMR-Centre for Ageing and Mental Health in Kolkata, India, with approval from the Research Integrity Office (RIO).
Numbers of new cases (incidence) and deaths (mortality) among older persons ≥60 yr, truncated age-standardized incidence & mortality rates (ASR per 100,000) for all cancer sites combined, site-wise, gender and world region-wise were reported, cancer predictions were estimated online using gco.iarc.fr portal8-10. The truncated ASR was calculated for the age group ≥60 yr by using the world standard population method proposed by Doll et al11. Mortality to incidence (M/I ratio) was calculated by dividing the mortality count by the incidence count and expressed in percentage. All the analysis was done using Microsoft Excel, IBM SPSS v21 (IBM, Armonk, NY, USA) and using IARC-WHO online portal (gco.iarc.fr, cancer today, cancer tomorrow and cancer over time).
Data permissionAll data were publicly available. However, necessary permission was obtained from IARC-WHO for data abstraction, analysis and reproducing tables and figures along with proper citation as per policy to use IARC data provided ( https://publications.iarc.fr/Terms-Of-Use ).
ResultsGlobally in 2020, an estimated 18.1 million persons were newly diagnosed with cancer, and 9.9 million (all cancers excluding non-melanoma skin cancer) died due to cancer in all age groups. Of these, 11.3 million cases, representing 62.3 per cent of all incidence cases and 7.5 million deaths, representing 71.2 per cent of all cancer-related deaths worldwide, were seen in the older age group.
Worldwide, older men accounted for an estimated 56.4 per cent of incidence cases and 56.6 per cent of deaths in 2020. The highest number of new cases and deaths (relative proportion) was seen in Asia, which accounted for 48.9 per cent of all global estimated cancer cases among older adults and 55.7 per cent of all global estimated cancer deaths among older adults. These findings were mainly due to population composition (Table I).
Table I. Incidence [cases (%), age-standardized rate] and mortality [deaths (%), age-standardized rate], Mortality-to-incidence ratio (M/I ratio) for all cancers (excluding non melanoma of skin) combined by sex and continents in 2020
Gender/world regions Incidence Mortality M/I ratio No. of cases, n (%) ASR No. of cases, n (%) ASR Both sexes Asia 5525124 (48.9) 879.2 3927273 (55.7) 616.1 71.1 Europe 2935714 (26) 1419.6 1623506 (23) 706.6 55.3 Northern America 1402737 (12.4) 1544.9 584062 (8.3) 576.7 41.6 Latin America & the Caribbean 855863 (7.6) 944.3 506178 (7.2) 531.7 59.1 Africa 458200 (4.1) 622.4 349421 (5) 479 76.3 Oceania 127874 (1.1) 1565.8 55741 (0.8) 602.5 43.6 World (both sexes) 11305512 (100) 1019.9 7046181 (100) 615 62.3 Male Asia 3211620 (50.3) 1095.2 2298840 (57.6) 782.4 71.6 Europe 1638004 (25.7) 1870.2 899659 (22.5) 956.6 54.9 Northern America 750824 (11.8) 1807.6 310078 (7.8) 686.2 41.3 Latin America & the Caribbean 472689 (7.4) 1178.2 271917 (6.8) 653.3 57.5 Africa 235527 (3.7) 714.8 178083 (4.5) 552.6 75.6 Oceania 72179 (1.1) 1871.2 31418 (0.8) 733.2 43.5 World (males) 6380843 (100) 1267.8 3989995 (100) 782 62.5 Female Asia 2313504 (47) 693.8 1628433 (53.3) 473.4 70.4 Europe 1297710 (26.4) 1080.1 723847 (23.7) 525.1 55.8 Northern America 651913 (13.2) 1321 273984 (9) 488.2 42 Latin America & the Caribbean 383174 (7.8) 759.6 234261 (7.7) 440.5 61.1 Africa 222673 (4.5) 553.1 171338 (5.6) 426 76.9 Oceania 55695 (1.1) 1290.6 24323 (0.8) 491.3 43.7 World (females) 4924669 (100) 815.7 3056186 (100) 481 62.1 Global cancer incidence rates by world region and genderThe global truncated ASR for ≥60 yr (male and female) were estimated as 1019.9 cases per 100,000 older populations and the mortality rate as 615.1 per 100,000 older populations. The highest incidence rate of cancer among the older aged population (male and female) was seen in Oceania (ASR, 1565.8 per 100,000), and the highest mortality rate was seen in Europe (706.6 per 100,000) (Table I).
Globally, the estimated age-adjusted incidence rate (ASR) for older men is 1267.8 cases per 100,000 elderly populations. The highest incidence rate of cancer was seen in Europe (1870.2 per 100,000), followed by Oceania (1871 per 100,000), Northern America (1807.6 per 100,000), Latin America and the Caribbean (1178.2 per 100,000), Asia (1095.2 per 100,000), and Africa (714.8 per 100,000)8-10.
The worldwide incidence rate for older women was estimated as 815.7 per 100,000 elderly women population and the highest age-adjusted incidence rate was seen in the Northern American (1321.0 per 100,000) countries, followed by Oceania (1290.6 per 100,000), Europe (1080.1 per 100,000), Latin America and the Caribbean (759.6 per 100,000), Asia (693.8 per 100,000) and Africa (553.1 per 100,000) (Table I).
Global cancer mortality rates by gender and world regionWorldwide the age-adjusted death rate for older men was estimated as 781.5 deaths per 100,000 with the highest in Europe (956.6 deaths per 100,000) followed by Asia (782.4 per 100,000), Oceania (733.2 per 100,000), North America (686.2 deaths per 100,000), Latin America and the Caribbean (653.3 per 100,000) and Africa (552.6 per 100,000) (Table I).
The age-adjusted death rate for older adult women globally was estimated at 480.6 deaths per 100,000 older women, with the highest being in European countries (525.1 per 100,000) followed by Oceania. North America (488.2 per 100,000), Asia (473.4 per 100,000), Latin America and the Caribbean (440.5 per 100,000), and Africa (426 per 100,000) (Table I).
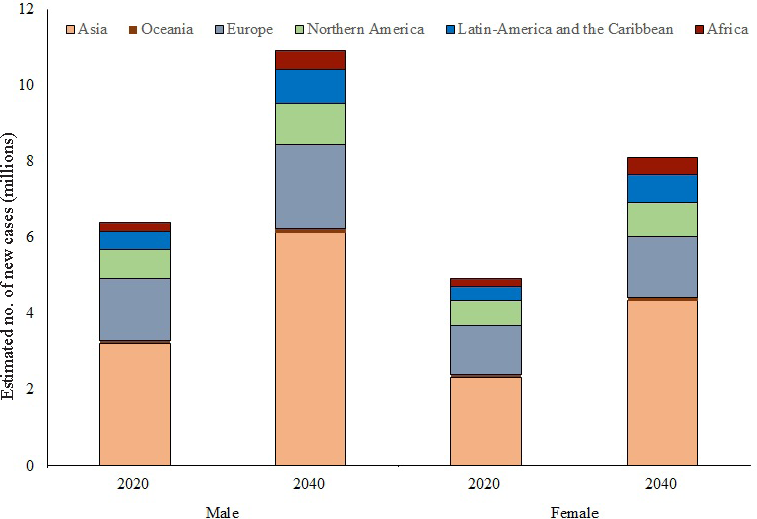
Future burden of cancer among older adultsOverall, the number of new among older adults is expected to rise 75.2 per cent by 2040 in older adults (male and female; Fig. 1) from 11.3 to 19.8 million; an expected 89.2 per cent relative increase in new cases in Asia, 29.7 per cent in Europe, 40.6 per cent in Northern America, 90.6 per cent in Latin America and the Caribbean, 106.1 per cent in Africa and 60.5 per cent in Oceania by 2040)8-10.
Export to PPT
The number of deaths among older adults is also expected to increase by 80.2 per cent worldwide (both sexes, from 7.05 to 12.7 million), with 93.7 per cent in Asia, 36.1 per cent in Europe, 97.4 per cent in Latin America and the Caribbean, 57.2 per cent in Northern America, 107.5 per cent in Africa, and 74.6 per cent in Oceania8-10.
Global comparison of mortality to incidence ratio (M/I) ratio by sex and world regionsThe M/I ratio, which provides a population-based indicator of survival was found to be highest for both males and females in Africa (76.3%) for older aged populations followed by Asia (71.1%), Latin America and the Caribbean (59.4%), Europe (55.3%), Oceania (43.6%) and lowest in Northern America (41.3%) (Table I).
Among older male adults worldwide, the mortality to incidence ratio was observed at 62.5 per cent. The highest M/I ratio percentage was seen in Africa at 75.6 per cent, followed by Asia (71.6%), Latin America and the Caribbean (57.5%), Europe (54.9%), Oceania (43.5%) and Northern America (41.3%). Among older female adults, the overall worldwide M/I ratio was observed at 62.1 per cent. Highest M/I ratio among older women is seen in Africa (76.9%) followed by Asia (70.4%), Latin America and the Caribbean (61.1%), Europe (55.8%), Oceania (43.7%) and Northern America (42%).
Global comparison of leading cancer incidence sites by genderGlobally among older males, prostate cancer was the leading cancer accounting for 19.1 per cent (1.22 million cases, 240.6 per 100,000) of all cases followed by lung (17.1%, 216.5 per 100,000), colorectum (12%, 152.1 per 100,000), stomach (8.2%, 103.4 per 100,000) and liver (5.8%, 74.5 per 100,000; (Table II)8-10.
Table II. Leading cancer incidence [number, relative (%), age-standardized rate] for all cancers combined (excluding nonmelanoma skin cancer) by sex in 2020
Incidence Male Female Number, n (%) ASR (world) Number, n (%) ASR (world) All cancers excluding NMSC (C00-97/C44) 6380843 (100) 1267.8 4924669 (100) 815.7 Breast (C50) 1027785 (20.9) 178.8 Prostate (C61) 1216139 (19.1) 240.6 Lung (C33-34) 1090137 (17.1) 216.5 593032 (12) 96.6 Colorectum (C18-21) 768791 (12) 152.1 634217 (12.9) 100.1 Stomach (C16) 521462 (8.2) 103.4 264551 (5.4) 41.9 Corpusuteri (C54) 232489 (4.7) 41.3 Pancreas (C25) 200758 (3.1) 39.4 196086 (4) 29.5 Liver (C22) 369121 (5.8) 74.5 195633 (4) 31.5 Cervixuteri (C53) 194195 (3.9) 35.1 Ovary (C56) 148463 (3) 25.6 Non-Hodgkin lymphoma (C82-86, C96) 173662 (2.7) 34.4 146784 (3) 23.7 Oesophagus (C15) 285875 (4.5) 57.7 136501 (2.8) 22.7 Thyroid (C73) 44991 (0.7) 9.3 121930 (2.5) 22.4 Bladder (C67) 358177 (5.6) 69.5 105942 (2.2) 16.2 Kidney (C64-65) 165306 (2.6) 33.2 102914 (2.1) 16.9Among elderly women, breast cancer (accounting for 20.9% of all cancer) was found as the leading cause of cancer, with ASR- 178.7 per 100,000, followed by colorectum cancer accounting 12.9 per cent (ASR 100.1 per 100,000), lung cancer accounting 12 per cent (ASR 96.6 per 100,000), stomach cancer accounting for 5.4 per cent (ASR 41.9 per 100,000) and corpus uteri cancer accounting for 4.7 per cent (ASR 41.3 per 100,000) (Table II)8-10.
In continent-wise analysis, it was observed that, among older male adults, prostate was the leading cause of cancer worldwide except Asia where lung cancer was the most common cancer. In older female adults, breast cancer was the leading cancer in all geographical regions (Table III)8-10.
Table III. Incidence [number, relative (%), age-standardized rate] for all cancers combined (excluding no melanoma skin cancer, NMSC) by sex and continents of world in 2020
Leading sites of incidence in 2020, ages 60+ (excl. NMSC), by Continents of world Male Female Site No Relative (%) ASR Site No Relative (%) ASR Asia Lung (C33-34) 652849 20.3 222.4 Breast (C50) 386691 16.7 121.9 Stomach (C16) 400427 12.5 136.4 Lung (C33-34) 312952 13.5 91.9 Colorectum (C18-21) 399826 12.4 136.3 Colorectum (C18-21) 307191 13.3 88.9 Prostate (C61) 340153 10.6 114.3 Stomach (C16) 184963 8 53.5 Liver (C22) 261875 8.2 89.9 Liver (C22) 129906 5.6 37.9 Oesophagus (C15) 224085 7 76.7 Cervixuteri (C53) 113770 4.9 36 Bladder (C67) 124134 3.9 42.1 Oesophagus (C15) 111023 4.8 33.1 Pancreas (C25) 95566 3 32.5 Pancreas (C25) 86747 3.7 24 Lip, oral cavity (C00-06) 74683 2.3 25.8 Ovary (C56) 68455 3 21.4 Non-Hodgkin lymphoma (C82-86, (C96) 74054 2.3 25.3 Corpusuteri (C54) 68191 2.9 21.9 Europe Prostate (C61) 411950 25.1 479.6 Breast (C50) 308729 23.79 276.4 Lung (C33-34) 252872 15.4 293.6 Colorectum (C18-21) 194621 15 150 Colorectum (C18-21) 228646 14 254.2 Lung (C33-34) 129380 9.97 111.1 Bladder (C67) 133925 8.2 144.2 Corpusuteri (C54) 89735 6.91 84.3 Stomach (C16) 66265 4 74.6 Pancreas (C25) 61525 4.74 44.4 Kidney (C64-65) 57924 3.5 68.1 Stomach (C16) 43005 3.31 32.1 Pancreas (C25) 56650 3.5 62.7 Ovary (C56) 42132 3.25 36.7 Melanoma of skin (C43) 48811 3 55.1 Non-Hodgkin lymphoma (C82-86, (C96) 40908 3.15 32.4 Non-Hodgkin lymphoma (C82-86, (C96) 45589 2.8 50.8 Bladder (C67) 39970 3.08 29.9 Liver (C22) 44909 2.7 51.1 Melanoma of skin (C43) 39843 3.07 33.9 Northern America Prostate (C61) 187597 25 482.6 Breast (C50) 169492 26 361.9 Lung (C33-34) 110173 14.7 257.3 Lung (C33-34) 105601 16.2 206.3 Colorectum (C18-21) 67498 9 160.9 Colorectum (C18-21) 61438 9.42 118.4 Bladder (C67) 60926 8.1 134.7 Corpusuteri (C54) 44698 6.86 101.4 Melanoma of skin (C43) 46268 6.2 106.5 Non-Hodgkin lymphoma (C82-86, (C96) 27628 4.24 53.2 Non-Hodgkin lymphoma (C82-86, (C96) 33116 4.4 76.7 Pancreas (C25) 25341 3.89 46.6 Kidney (C64-65) 31350 4.2 77.5 Melanoma of skin (C43) 24904 3.82 50.6 Leukaemia (C91-95) 27842 3.7 63.7 Leukaemia (C91-95) 19618 3.01 36.5 Pancreas (C25) 27003 3.6 62.8 Kidney (C64-65) 18982 2.91 39.3 Liver (C22) 24652 3.3 63 Bladder (C67) 18223 2.80 32.9 Latin America and the Caribbean Prostate (C61) 180204 38.1 452.9 Breast (C50) 93942 24.52 197.1 Colorectum (C18-21) 46488 9.8 115.4 Colorectum (C18-21) 47430 12.38 89.6 Lung (C33-34) 45724 9.7 113.1 Lung (C33-34) 30631 7.99 59.7 Stomach (C16) 29380 6.2 72.1 Cervixuteri (C53) 20770 5.42 43 Bladder (C67) 20299 4.3 49.3 Corpusuteri (C54) 18788 4.90 40.3 Liver (C22) 16159 3.4 39.7 Stomach (C16) 18678 4.87 34.6 Pancreas (C25) 13791 2.9 33.9 Pancreas (C25) 15235 3.98 28 Kidney (C64-65) 12784 2.7 32.8 Liver (C22) 14014 3.66 26.2 Non-Hodgkin lymphoma (C82-86, (C96) 10591 2.2 26.7 Thyroid (C73) 12444 3.25 27.8 Oesophagus (C15) 9706 2.1 24.2 Ovary (C56) 10611 2.77 21.8 Africa Prostate (C61) 77375 32.9 236 Breast (C50) 55035 24.72 137.1 Lung (C33-34) 20728 8.8 63.2 Cervixuteri (C53) 35172 15.8 87.4 Liver (C22) 19547 8.3 58.6 Colorectum (C18-21) 16148 7.25 39.9 Colorectum (C18-21) 17746 7.5 53.7 Liver (C22) 13881 6.23 34.4 Bladder (C67) 16032 6.8 49.4 Ovary (C56) 8654 3.89 21.5 Stomach (C16) 9858 4.2 29.8 Stomach (C16) 8436 3.79 20.9 Oesophagus (C15) 7826 3.3 23.5 Corpusuteri (C54) 8322 3.74 20.7 Non-Hodgkin lymphoma (C82-86, (C96) 7205 3.1 21.5 Lung (C33-34) 8059 3.62 19.9 Pancreas (C25) 5662 2.4 17.2 Oesophagus (C15) 7448 3.34 18.4 Leukaemia (C91-95) 5073 2.2 15.4 Non-Hodgkin lymphoma (C82-86, (C96) 6908 3.1 17.2 Oceania Prostate (C61) 18860 26.1 515.3 Breast (C50) 13896 24.95 351.4 Colorectum (C18-21) 8587 11.9 215.6 Colorectum (C18-21) 7389 13.27 155.9 Melanoma of skin (C43) 7960 11 202.9 Lung (C33-34) 6409 11.51 145.5 Lung (C33-34) 7791 10.8 196.2 Melanoma of skin (C43) 5080 9.12 116.4 Non-Hodgkin lymphoma (C82-86, (C96) 3107 4.3 78.8 Corpusuteri (C54) 2755 4.95 71.3 Bladder (C67) 2861 4 66.3 Non-Hodgkin lymphoma (C82-86, (C96) 2207 3.96 49.8 Kidney (C64-65) 2522 3.5 66.7 Pancreas (C25) 2046 3.67 42.3 Leukaemia (C91-95) 2299 3.2 57 Leukaemia (C91-95) 1490 2.68 32 Pancreas (C25) 2086 2.9 51.3 Kidney (C64-65) 1265 2.27 29.3 Liver (C22) 1979 2.7 55 Thyroid (C73) 1230 2.21 33.3 Global comparison of leading cancer mortality sites by genderLung cancer accounted for 23.4 per cent of all cancer deaths among older men, followed by colorectum cancer 10.2 per cent, stomach 9.5 per cent, prostate 9 per cent, and liver 8.6 per cent. The highest proportion of the relative burden of lung cancer death was seen in Asia (25.1%) followed by North America (23.9%), Europe (23.9%) and Oceania (19.2%) and prostate cancer was observed as the leading cause of death among elderly in Africa (24%) and Latin America and the Caribbean (20.3%).
Globally, the leading cause of death among elderly men is observed was lung cancer (184.2 deaths per 100,000) followed by cancer of colorectum (78.5 deaths per 100,000), stomach (74.6 deaths per 100,000), liver (69.1 deaths per 100,000) and prostate (66.7 deaths per 100,000). Estimated age-standardized mortality rates comparison showed that globally among elderly males lung cancer is estimated as the leading cause of death in 90 countries, followed by prostate in 75 countries, lung cancer was estimated as the leading cause of death in 90 countries, followed by prostate cancer in 75 countries, the stomach cancer in nine countries and liver cancer in eight countries8-10. Among older adult women, 15.9 per cent of all deaths were due to lung cancer, followed by breast cancer 13.2 per cent, and cancer of colorectum 11.2 per cent, stomach cancer 6.5 per cent and pancreas 6.2 per cent.
Age-standardized comparison of death rates showed, among older women lung cancer (77.2 deaths per 100,000) had the highest death rate followed by breast (65.2 per 100,000), colorectum (49.6 per 100,000), stomach (30.8 per 100,000), liver (29.3 per 100,000) and pancreas (28.0 per 100,000) (Table II). Among elderly females, breast cancer the leading cause of death in 82 countries was followed by cervix uteri in 43 countries, lung in 38 countries, liver in eight countries and colorectum in seven countries8-10.
In region-specific analysis, breast cancer was found to be the top leading cause of death in Africa (18.2%), followed by Latin America and the Caribbean (14.1%) and Europe (15.3%), whereas contrastingly, lung cancer was observed as the top leading cause of death in Northern America (24.3%), followed by Asia (17%) and Oceania (18.1%)8-10.
Future burden of cancer by sitesGlobally leading future burden of new cases among older adults is expected due to lung cancer (male and female), it is estimated to increase from 1.68 to 2.97 million (76.4%) by 2040, prostate cancer among older males by 78.7% (from 1.22 to 2.17 million cases), breast in older female adults will rise from 1.03 to 1.71 (66.3%), cervix uteri from 0.19 to 0.31 million, and stomach in both gender (male and female) will rise from 0.79 to 1.4 million (77.6%)8-10. Globally leading future burden of death among older adults also was estimated due to lung cancer (male and female), which will rise from 1.42 to 2.53 million (78.4%), followed by deaths due to stomach cancer will increase from 0.58 to 1.04 million (79.5%), liver 0.53 to 0.92 million (75.1%), prostate in men 0.36 to 0.72 million (100.4%), breast 0.4 to 0.7 million (73.6%)8-10.
DiscussionAgeing is one of the important non-modifiable biological risk factors for developing cancer12. Previous studies have shown that the older person has an 11 times higher risk of developing cancer as compared to the younger ones13. Older patients are always at an elevated risk of unfavourable outcomes due to co-existing co-morbidity conditions14. Lower survival rates were seen in older adults as compared to the younger ones due to co-existing co-morbidity conditions and limited treatment options15,16. An analysis done on American cancer patients revealed that only 65 per cent of those who were 85 years of age or older received surgical treatment15.
Worldwide, an estimated 62.3 per cent of all incidence cases and 71.2 per cent of all cancer-related deaths worldwide were seen among older adults in 2020; a similar study also reported 66.3 per cent burden16. Of all global burdens among older adults, about half of the cancer incidence cases were 48.9 per cent and more than half (55.7%) of all cancer-related deaths among older were seen in Asian countries. A previous study on older adults estimated that 55.6 per cent of older cases were from LMICs17. It was also quite significant to come across from the present study that China alone accounted for 30.5 per cent of all global deaths due to cancer among older adults.
The number of new cancer cases among older adults is expected to rise from 11.3 to 19.8 million (a 75.2% increase). A study done by Pilleron et al17, also reported a 78 per cent increase in older adult cases worldwide and an expected increase of 84 per cent in LMICs17.
Lung cancer is estimated as the leading cause of death in both male (90 countries) and female (38 countries) older adults. Mainly higher incidence and mortality rates were seen in Eastern Asia, Central and Southern Europe, Northern America and Australia/ New Zealand. In high-income countries, smoking is the leading cause of lung cancer, and is responsible for about two-thirds of deaths due to lung cancer18, which can be easily prevented through tobacco policies and regulations.
In China, it is observed that lung cancer among older women has the highest incidence rate in the country, whereas globally breast cancer is the leading global cause of cancer among elderly women. This may be due to second-hand smoke or indoor air pollution, as smoking rates are lower among older Chinese women. The use of smoky coal relative to smokeless coal increased risk by about 99 times among Chinese women19. Fine particulate matter (PM2.5), an air pollutant, is one of the main factors attributing largely to the proportion of lung cancer deaths apart from smoking, and the PM2.5 ranges from 4.7 per cent in the United States to 20.5 per cent in China20.
While prostate and lung cancer are the leading causes of cancer among older men globally, contrary to that in India, lip and oral cavity cancer are the leading causes. This may be due to the high prevalence of smoking and smokeless tobacco consumption and its prolonged lifetime impact21. According to the Global Adult Tobacco Survey (GATS 2016-2017)22, the prevalence of tobacco consumption in India, either smoked or smokeless form, among adults is estimated as 28.6 per cent; in males, it is 42.4 per cent and 14.2 per cent in women. According to the population-based cancer registry report of India tobacco-related cancer in India ranges from 24.5 per cent to 70.4 per cent in males and 10.1 per cent to 46.5 per cent in females23.
Breast cancer among older adult women is the leading cause of cancer in 145 countries and is the first or second leading cause of mortality in 156 countries. The burden is increasing in countries with demographic and socio-economic transitions like Asian countries, South America and Africa3. Studies have shown that in Asia and African countries, women developed breast cancer at least 10 years earlier than in the most part of Europe or America24. As these countries have younger age groups compared to others, which suggests that in the coming decade as the population will be ageing, the burden will be shifted towards these countries.
The M/I ratio is estimated at 62.3 per cent worldwide, whereas the highest is seen among African countries (76.3%) followed by Asian Countries (71.1%) and the lowest is observed in Northern America (41.6%). The M/I ratio can be considered a comparative indicator of disparities in cancer outcomes and treatment availability25,26. In lower or lower-medium-income countries, the estimated higher M/I ratio is a matter of concern, and necessary cancer prevention and care plan needs to be adopted. According to the Lancet commission report 2018, 80 per cent of patients living in lower-medium-income countries have very limited or no access to pain and palliative care relief27.
Cancer treatment and care of older patients is challenging for both treating doctors and family members because older adults are more likely to have chronic health conditions, higher treatment-related toxicities and complications, etc28,29. The increased burden among older adults will challenge the worldwide strained healthcare systems, especially in developing countries and bring economic costs to the countries.
As the global burden of cancer is increasing, mainly among older adults due to the interplay between ageing and other risk factors, the role of geriatric oncology has become immense30. The incidence and mortality pattern is diverse geographically; a local comprehensive geriatric cancer control strategy is therefore the need of the hour. Geriatric oncology attempts to ensure overall improvement in functional and nutritional status, social support, cognition, and psychosocial functioning of elderly cancer patients.
Geriatric oncology has paramount importance, especially in lower- medium- income countries like India, where it is seen that 98 per cent of older patients have at least one deficit, of which co-morbidities (79%) is very common followed by fatigue (77%), nutritional deficiency (65%), functional deficiency and falls (52%) and psychological issues (32%)31. Psychological aspects of cancer patients are often neglected. Studies showed about 30-40 per cent of older aged cancer patients needed psychological counselling. However, most countries do not integrate psychological counselling into their treatment plan32. Along with psychological counselling, social support and nutrition counselling are to be provided for better outcomes33. Geriatric assessment and appropriate interventions are crucial in improving the overall health and wellbeing. However, limited utilization of this is observed among lower or lower-medium-income countries.
Due to the non-inclusion of elderly adults in randomized trials, there was a lack of evidence on risk and benefits. For example, due to restrictions on breast cancer screening for elderly females above 75 years, the risk-benefit assessment could not be done, ultimately impacting the treatment outcomes34,35. Studies also supported the necessity of stoppage of smoking or alcohol cessation, weight management, and social support for overall health benefits for older adults36,37.
The limitations of our study should be taken into consideration when interpreting the results. Firstly, not all countries have the same quality of data, particularly those where there isn’t a high-quality national mortality register, which may affect the estimations. Secondly, country-specific reasons of death were not available, to associate causes with the mortality rates. Moreover, in the GLOBOCAN 2020 online database, for some countries, data were not available for incidence and mortality estimates, so under- or over-estimation cannot be ruled out. However, despite the limitations IARC-WHO is a trustworthy worldwide data source for to comprehend the pattern of cancer statistics.
Overall, with disparity, a 2-3 fold increase in cancer incidence (75.2% increase) and mortality (an 82.8% increase) is estimated among older adults by 2040. A comprehensive geriatric treatment protocol needs to be adopted as per local situation, along with a global action plan to deal with the growing cancer burden in older adults.
留言 (0)