
記住我



The average age of patients admitted to the intensive care unit was 77.2 ± 9.9 years. The study included 78 patients, including 42 females (53.8%) and 36 males (46.2%). Comorbidities were present in significant proportions, with 24 patients (30.8%) suffering from diabetes, 23 (29.5%) from hypertension, 14 (17.9%) from heart disease, 20 (25.6%) from COPD, 11 (14.1%) from malignant tumors, and 28 (35.9%) exhibiting neurological comorbidities. The median Nutric score was 6, segregating the cohort into 31 patients (39.7%) with low scores and 47 patients (60.3%) with high Nutric scores. Critical interventions were common, with 48 patients (61.5%) necessitating the use of vasoactive drugs and 18 (23.1%) receiving renal replacement therapy. Upon admission to the intensive care unit, 52 patients (66.7%) required mechanical ventilation, and 32 (41.0%) were diagnosed with acute kidney injury. The median duration of hospital stay was 14 days (refer to Table 1 for additional details).
Table 1 Descriptive statistics of demographic and clinical characteristics in intensive care unit patients and pairwise comparisons in terms of mortality during follow-upDuring the observation period in the intensive care unit, several factors were significantly associated with higher mortality rates. These included older age, a greater incidence of diabetes mellitus (DM), greater nutritional score values, a greater proportion of patients with elevated nutritional scores, increased utilization of vasoactive drugs, more frequent renal replacement therapy, a greater incidence of mechanical ventilation requirements, a greater occurrence of acute kidney injury, and extended hospital stays (p < 0.05 for all mentioned parameters). In contrast, factors such as sex and the presence of other comorbidities, including hypertension (HT), cardiac disease, chronic obstructive pulmonary disease (COPD), malignant tumors, and neurological disorders, were not significantly different between the nonsurvivor and survivor groups (p > 0.05 for each). These findings further emphasize the multifactorial nature of outcomes in intensive care settings (detailed statistics are available in Table 1).
Notably, hemoglobin and albumin levels were significantly lower in the nonsurvivor group than in the survivor group (p = 0.009 and p < 0.001, respectively). In contrast, other hematological and biochemical indices did not significantly differ between the groups (p > 0.05 for each), underscoring the particular impact of specific nutritional and hematological factors on patient outcomes (refer to Table 2 for a detailed breakdown).
Table 2 Descriptive statistics of hematological and biochemical parameters in ICU patients and pairwise comparisons for mortality during follow-upPatients in the intensive care unit with higher Nutric scores demonstrated a significantly increased incidence of acute kidney injury, the need for vasoactive drugs, and the need for mechanical ventilation. Furthermore, these patients exhibited a markedly higher mortality rate (p ≤ 0.001 for each of these criteria). (Table 3).
Table 3 Comparison of mortality and serious clinical parameters according to nutric score categoriesThe predictive capacity of the Nuntric score was evaluated through receiver operating characteristic (ROC) analysis, which revealed substantial prognostic efficacy across multiple critical conditions. For mortality prediction, an AUC value of 0.788 was achieved, indicating a high level of accuracy. When a cutoff value of > 5 was used, the model demonstrated an accuracy rate of 76.92%, with a PPV of 70.21%, an NPV of 87.10%, a sensitivity of 89.19%, and a specificity of 65.85% (p < 0.001), highlighting its reliability in clinical scenarios (Table 4).
Table 4 ROC Analysis Outcomes of Nutrition Assessment Score for various clinical endpointsSimilarly, the need for vasoactive drug use was effectively predicted, with an AUC of 0.772. With a more conservative cutoff of > 4, the predictive model maintained a robust accuracy rate of 78.21%, a PPV of 79.25%, an NPV of 76.00%, a sensitivity of 87.50%, and a specificity of 63.33% (p < 0.001), confirming its utility in predicting this specific intensive care requirement (Table 4).
The analysis extended to the prediction of mechanical ventilation necessity, where the model exhibited an AUC of 0.739. With a cutoff value of > 5, the accuracy rate was 73.08%, complemented by a PPV of 82.98%, an NPV of 58.06%, a sensitivity of 75.00%, and a specificity of 69.23% (p = 0.001), indicating a balanced predictive capability (Table 4).
Finally, the forecast of acute kidney injury had an AUC of 0.674. At a similar cutoff value of > 5, the model’s accuracy was slightly moderated at 67.95%, accompanied by a PPV of 57.45%, an NPV of 83.87%, a sensitivity of 84.37%, and a specificity of 56.52% (p = 0.004) (Table 4).
A comprehensive logistic regression analysis was conducted to ascertain the influences of the nutritional score and various clinical conditions on mortality outcomes in intensive care unit patients. The univariate analysis revealed significant associations between mortality and several key factors, including albumin levels, vasoactive drug utilization, the need for mechanical ventilation, and classification within the high nutritional score category (p < 0.001 for each). Remarkably, a one-unit elevation in the serum albumin concentration correlated with a 22% decrease in mortality risk. Conversely, the initiation of vasoactive drugs, the imposition of mechanical ventilation, and inclusion in the high nutritional score bracket were implicated in mortality risk increases by factors of 7.29.
Subsequent multivariate analyses nuanced these findings. While the use of vasoactive drugs diverged significantly (p = 0.927), the remaining variables preserved their critical roles. Specifically, each unit increase in the serum albumin concentration was associated with a 19% reduction in mortality. In stark contrast, the necessities of mechanical ventilation and categorization in the high-Nutric score echelon were potentiated, increasing mortality risk by 8.11 and 9.79 times, respectively.
These insights, consolidated in Table 5, underscore the multifaceted nature of mortality determinants in intensive care contexts, with nutritional status, emergent clinical interventions, and severity assessments via the Nutric score proving pivotal.
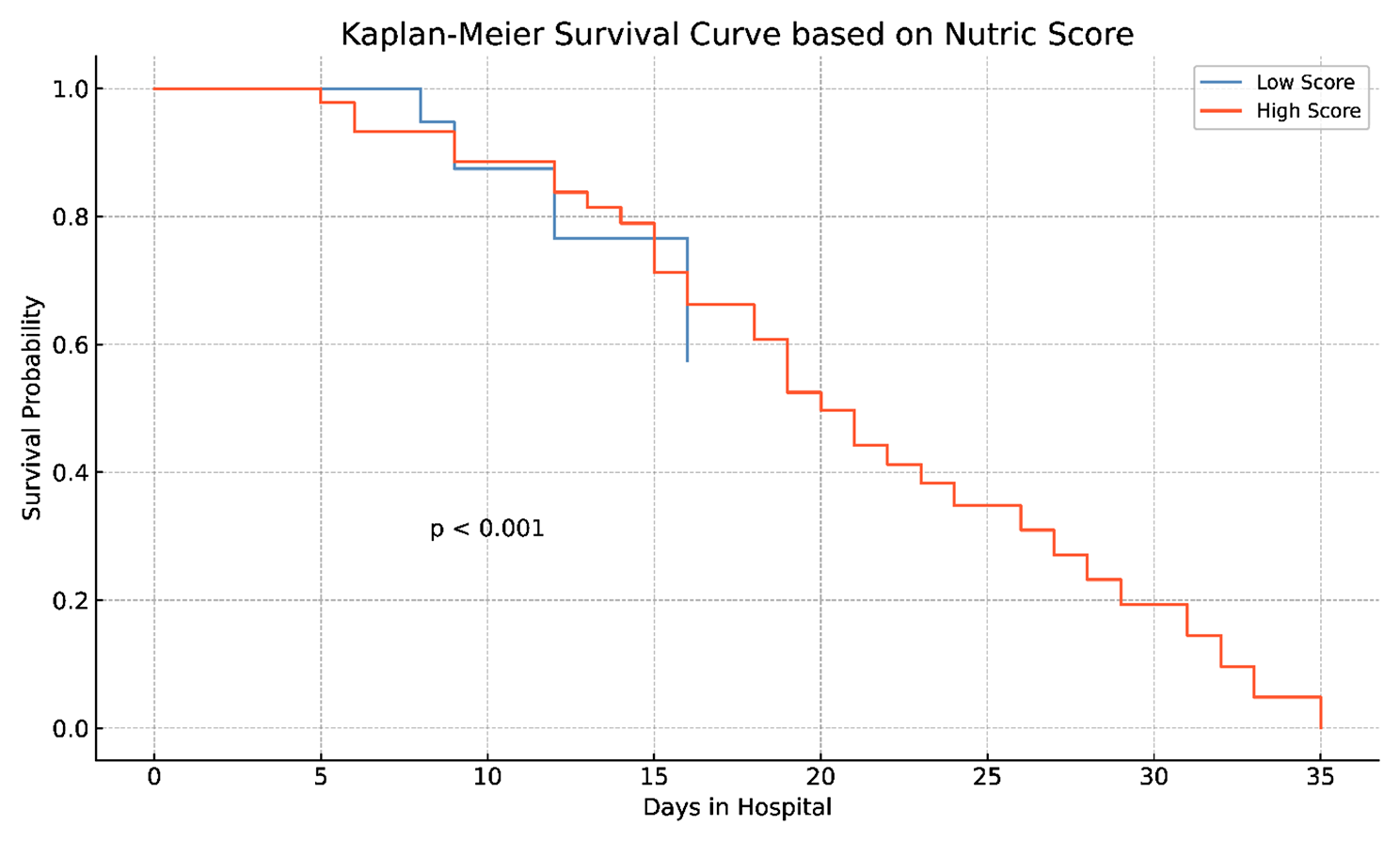
Table 5 The effect of nutric score and clinical conditions on mortality in intensive care unit patientsAs depicted in Fig. 1, the Kaplan‒Meier survival curves distinctly demonstrate a significant divergence in survival probabilities within the intensive care context, contingent upon patients’ Nutric scores. Notably, individuals with lower nutritional scores had a greater likelihood of prolonged survival than did those with elevated scores (p < 0.001). This statistically significant disparity, derived from Kaplan‒Meier analysis, highlights the critical prognostic implications of Nutric scores, suggesting their consideration as substantial determinants in patient survival projections and consequent healthcare strategizing within intensive care units.
Fig. 1
K‒M survival curves for intensive care unit survival times in the low- and high-nutrient score groups
留言 (0)