Participants
This single-blind, randomized controlled clinical trial was prospectively registered at the Chinese Clinical Trial Registry (ChiCTR2300076209, registration date: 27/9/2023) and was conducted at Anqing Medical Center of Anhui Medical University (Anqing Municipal Hospital) from October 1, 2023, to February 29, 2024. The study protocol was approved by the Ethics Committee of Anqing Medical Center of Anhui Medical University. Written informed consent was obtained from each selected patient before surgery. Our study followed the Consolidated Standards and Regulations.
Following ethics approval and informed consent, CRS subjects were prospectively enrolled following the following criteria: synchronous sinonasal symptoms present for more than 12 weeks, sinusitis evidenced by a sinus computerized tomography (CT) scan, age between 18 and 65 years, American Society of Anaesthesiologists (ASA) physical status I or II, and scheduled for elective FESS. The exclusion criteria included patients with systemic diseases (including neuropsychiatric diseases, respiratory diseases,circulatory disease,etc.), hypovolemia, bradycardia (HR < 50 beats per minute or lower), second- or third-degree atrioventricular blockage, BMI > 30 kg/m2, a recent history of acute upper respiratory tract infection or pulmonary infection, the use of any sedative before surgery, a history of food and drug allergy, opioid medication misuse, and a refusal to participate in the study.
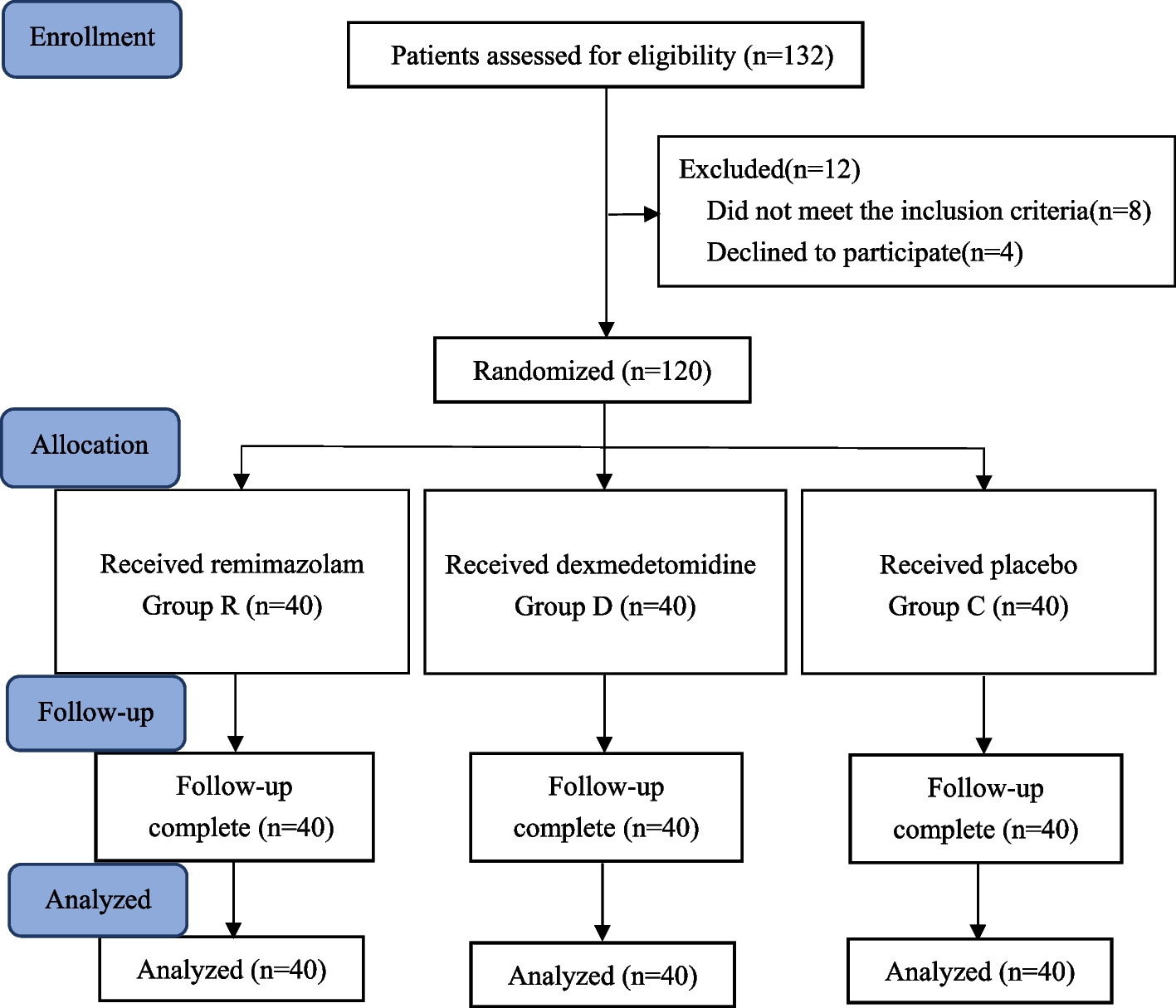
A total of 120 patients eligible for this study were randomized to Group R, Group D or Group C with a 1:1:1 allocation. Block randomization was performed via a computer-generated random table. Given the complete difference in infusion protocols among the three groups, the clinical trial was a single-blinded study. The medical care personnel and researcher staff who performed the infusion protocols could not remain blinded to the study group allocation. However, all eligible participants, data collectors and assessors of the study outcomes were independent. Details of the QoR-40 scale, visual analogue scale (VAS) score and postoperative nausea or vomiting (PONV) intensity were explained to each patient 1 day before surgery. The patients were not given any preoperative medication.
Study protocol
Standard monitoring, including electrocardiography (ECG), heart rate (HR), mean arterial pressure (MAP), and the peripheral pulse oximeter value (SPO2), was monitored throughout the procedure (Philips MX500, Boeblingen, Germany). In Group D, a loading dose of 1.0 µg/kg dexmedetomidine was infused over 10 min before anaesthesia induction, followed by maintenance infusion at 0.5 µg/kg per hour until the end of surgery. In Group R, a loading dose of 0.075 mg/kg for remimazolam was infused over 1 min before anaesthesia induction, followed by a maintenance infusion at 0.1 mg/kg per hour until the end of surgery, and the infusion was stopped when hypotension (MAP less than 60 mm Hg) occurred. Patients in Group C were given the same amount of placebo equal to dexmedetomidine. Anaesthesia was induced with propofol (2.0 mg/kg), sufentanil (0.5 µg/kg), and cisatracurium (1.5 mg/kg). After endotracheal intubation (ID:7.5 mm or 7.0 mm), anaesthesia was maintained with propofol and remifentanil at the effect site, followed by target-controlled infusion (TCIs) of propofol and remifentanil via a TCI pump. The initial TCI levels of plasma propofol and remifentanil were set as 3.0 μ g/ml and 5.0 μ g/ml, respectively. Mechanical ventilation was applied in volume-control mode with a tidal volume (VT) of 8–10 ml/kg at a respiratory rate (RR) of 10–12 beats per minute (bpm) to provide an end-tidal carbon dioxide concentration of 35–45 mm Hg. The inspired oxygen fraction (FiO2) was 0.5 (balanced with air) throughout the anaesthesia period. The depth of anaesthesia was maintained at a BIS range between 45 and 60, as were the mean arterial pressure and heart rate within 20% of the baseline values, by adjusting the TCI concentration of plasma propofol and remifentanil during surgery. Atropine (0.5 mg) was intravenously injected to treat bradycardia. Cisatracurium 2.0 to 4.0 mg was intermittently used for muscle relaxation, and all surgeries were performed by the same team. The operating table was placed in the 15-degree reverse Trendelenburg position during surgery. To prevent PONV, ondansetron (4 mg) was administered intravenously 10 min prior to the end of surgery. After surgery, all patients were transferred to the postanaesthesia care unit (PACU), with the endotracheal tube retained. The endotracheal tube was removed after full return of consciousness and spontaneous ventilation, and the train-of-four ratio was ≥ 0.9. The discharge criteria from the PACU included stable vital signs, a pain score of 2 or less, the absence of PONV, and a calm and alert patient. If the visual analogue scale (VAS) score exceeded 3,intravenous tramadol 50 mg served as rescue analgesia.
Data collection
The main goal of this study was to assess the global QoR-40 score 3on the day before surgery and postoperative Day 1 (POD1), which includes five dimensions: emotional state (9 items), physical comfort (12 items), physical independence (5 items), psychological support (7 items), and pain (7 items),and each item is rated on a 5-point numerical scale, the score of the QoR-40 ranges from 40 to 200, and the recovery state is proportional to the score (40 = extremely poorest recovery quality, 200 = best recovery quality) [3]. Demographic variables such as sex, age, height, weight and ASA score were recorded. Haemodynamic parameters, including MAP and HR, were measured and recorded before anaesthesia induction (T0), before intubation (T1), immediately after intubation (T2), at the end of surgery (T3), immediately after extubation (T4), and upon PACU arrival (T5). The durations of anaesthesia and surgery were recorded. The cumulative consumption of propofol and remifentanil during surgery was recorded. The time to return of consciousness, which was calculated from the time of stopping narcotic agent infusion until sustained eye opening (for > 5 s), and the length of stay at the PACU were documented. The time to first rescue analgesia was recorded. The maximal VAS pain scores in the PACU and ward were measured with the VAS scale; this 10-point scale ranges from 0 (no pain) to 10 (the most pain imaginable) [11]. The level of sedation upon PACU arrival was documented via a 10-point Richmond Agitation Sedation Scale (+ 4 = combative, -5 = unarousable) [12]. PONV( assessed by a verbal descriptive scale as 0: no nausea, 1: mild nausea, 2: moderate nausea, 3: severe nausea and vomiting) [13], the need for vasopressors, and prolonged respiratory support were recorded.
Statistical analysis
As described by Hu et al. [14], the calculation of sample size was based on the quality of recovery on the day before surgery and postoperative Day 1. The allowable error was 0.05, and each group needed 36 patients (assuming a power of 80%). Forty patients were included per group, resulting in a 10% dropout rate. Data analysis was performed via SPSS version 23.0 (SPSS Inc., Chicago, IL). The Shapiro‒Wilk test was used to evaluate the normal distribution of the data. Continuous variables are presented as the mean (standard deviation, SD). Normally distributed variables were compared via Student’s t test. Nonnormally distributed variables are presented as the median and interquartile range [M (IQR)] and were compared via the Kruskal–Wallis H test. Qualitative data are presented as numbers or percentages and were compared via the chi-square test. P values of less than 0.05 were considered statistically significant.




留言 (0)