
記住我



This pilot randomized controlled trial was conducted at Ningbo No.2 Hospital (Ningbo, China) from March 2023 to June 2023. The study protocol was approved by the Clinical Research Ethics Committee of the Ningbo No.2 Hospital (Approval NO.SL-NBEY-KY-2022-061-01) and the study was registered with ClinicalTrials. gov (ChiCTR2300067437). Trainees were randomized to either the intervention or control group. The randomization process was conducted by an anesthesiologist (not involved in assessing outcomes) using a random numbers table. All subjects, patients and anesthesiologists, provided written informed consent.
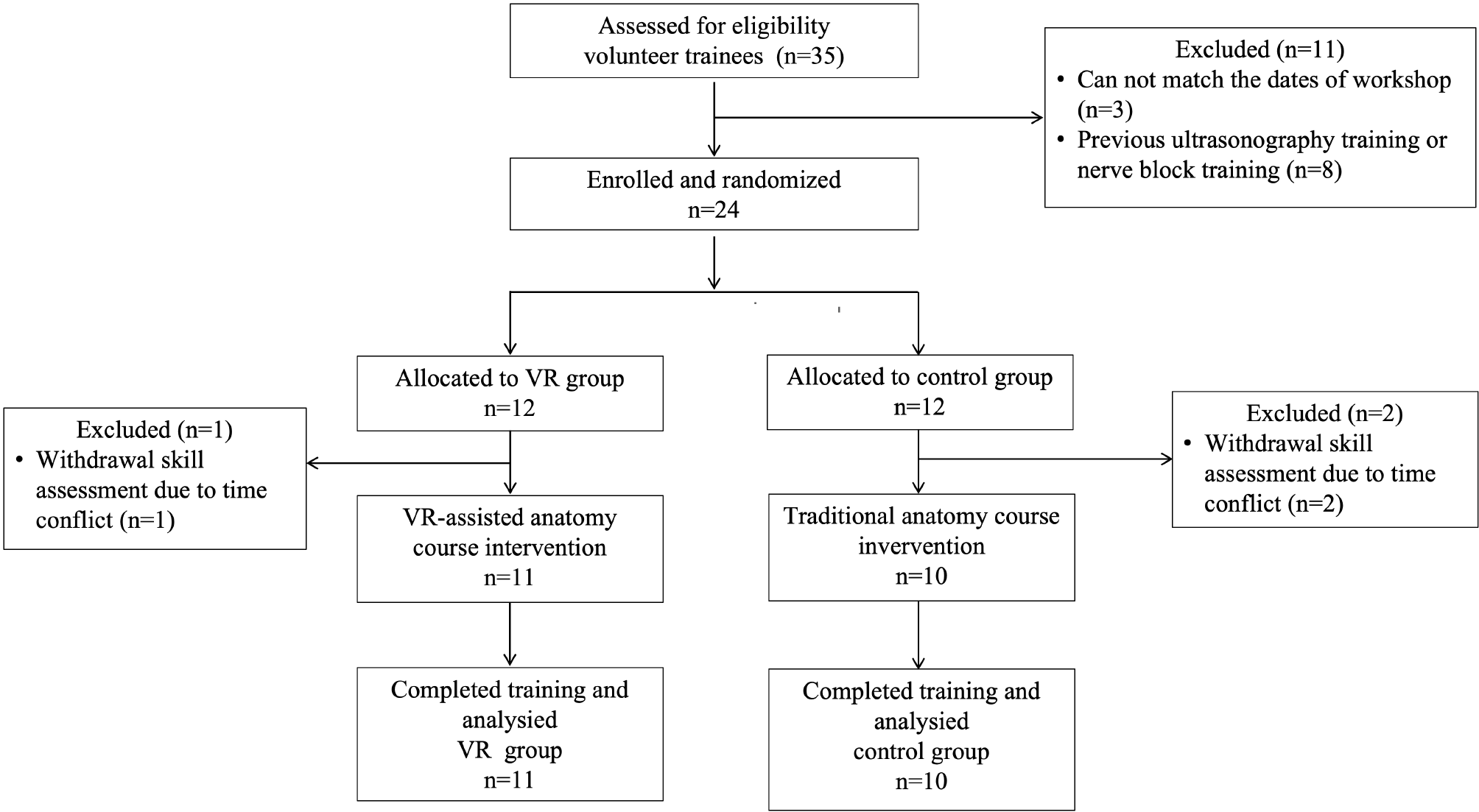
Study populationThis study enrolled fifth-year medical students and first-year residents both majoring in anesthesiology who were on rotation at Ningbo No.2 Hospital and had completed all human anatomy courses in undergraduate education stage. All participants had completed at least a 3-month rotation in anesthesiology and had prior experience in venous and arterial catheterization. Our exclusion criteria were previous nerve block experience or any ultrasonography/UGNB training. A total of 24 participants were recruited on a volunteer basis and allocated into two groups: a VR group (VG) (n = 12) and a control group (CG) (n = 12). 3 participants dropped out (1 from the intervention group and 2 from the control group) due to time conflict with the skill assessment. A total of 21 participants were analyzed in this study. (Fig. 1). All trainees in both groups took part in a workshop designed for ultrasound-guided interscalene brachial plexus block. For VG, trainees received a VR-integrated course. In contrast, trainees in CG completed the course without VR.
Concurrently, patients under 60 years of age scheduled for shoulder or upper limb surgeries without significant neck pathologies were recruited in the phase of outcome assessment.
Research objectivesThe primary objective was to evaluate the effectiveness of VR-facilitated anatomy education in the first performance of ultrasound-guided interscalene brachial plexus blockade among novice anesthesiologists. Secondary objectives included assessing the improvement in theoretical knowledge using VR in educational methods.
Fig. 1 Curriculum design
Curriculum designThe curriculum of UGNB training was structured around a 3-hour practical workshop, divided into two distinct stations, in combination with evaluations on theoretical knowledge and skills performance (Fig. 2). In the first station, all participants received a 90-minute theoretical course with reading material in advance. During that course, all participants were provided with a 60-minute lecture presented by one expert, imparting knowledge of ultrasound-guided interscalene brachial plexus block in a PowerPoint presentation (including anatomy, ultrasound imaging, indications, contraindications, technique, and potential complications), and a 10-minute video of an expert anesthesiologist explaining and performing nerve block was played. A pivotal distinction was introduced between the VR group and the control group: the former engaged in a 20-minute immersive VR experience using VR anatomy software, while the later was presented with 2D pictures. Participants in VR group could directly manipulate the VR model with controllers by using a head-mounted display (Fig. 3).
Fig. 2 Fig. 3
Fig. 3
(A) An anesthesiology trainee learning the anatomy of brachial plexus through VR glasses and controllers (Oculus Quest 2); (B) (C) (D) Screenshots of anatomy learning of brachial plexus in 3D Organ Anatomy
In the second station, a hands-on 90-minute practical session was conducted. All participants in both groups practiced ultrasonographic scan on the neck of volunteers under the instruction of an expert within 60 min, ensuring that everyone knew how to correctly identify target structures in the checklist and acquire ultrasound images. A checklist of anatomical structures (Appendix A) was provided according to an international consensus on anatomical structures to identify on ultrasound for the performance of basic blocks in ultrasound-guided regional anesthesia [8]. Followingly, participants in both groups completed a 30-minute ultrasound-guided block practice on a nerve block model.
Materials and equipmentIn this study, 3D Organon Anatomy® (Medis Media, Queensland, Australia) was used for anatomy training in the VR group. This software provides VR anatomical models within immersive environments combing with a 3D glass and offers the ability to transect anatomical models in any angle by a VR controller. The VR hardware used in this study was the Oculus Quest 2 headset and hand controllers (Oculus Rift®; Oculus VR, Irvine, CA). The anatomical region used for training was determined as the brachial plexus module and the neck region module in 3D Organ Anatomy. The ultrasonography equipment used in the study was the Sonosite SII (FUJIFILM Sonosite Inc.) The ultrasound-guided nerve block puncture training model (Ningbo Lancet Company) was constructed from an elastomeric tissue-mimicking material that facilitates needle insertion and ultrasonographic visualization. The model was equipped with four nerves, each with an internal diameter of 2–3 mm and a depth of 10–20 mm. The dimensions of the model are 150 mm* 120 mm*40 mm (length*width*height).
Evaluation of performanceThe outcomes were evaluated through a two-phase testing process (Fig. 2). The primary outcome was the trainees’ performance during their initial ultrasound-guided interscalene brachial plexus block, assessed using both the Global Rating Scale (GRS) and a task-specific Checklist (see Appendix B). The improvement in scores for theoretical knowledge measured by written multiple-choice questions (MCQs) (see Appendix C) was the secondary outcome.
Phase I: theoretical tests. Participants completed written MCQs testing their knowledge of both anatomy and ultrasound before and after the theoretical course on ultrasound-guided brachial plexus block. The questions on both MCQs tests were based on the lecture. Two different tests, each with 20 questions, scores ranging from 0 to 100, were employed. The pre-test and post-test were compared separately between VG and CG. The score gains of both groups were compared as well. Both MCQs tests had previously been employed as part of UGNB training within our department. In this study, the pre-test and post-test of MCQs had difficulty indices of 0.5 and 0.57, and discrimination indices of 0.2 and 0.25, which were consistent with standard metrics for effective assessment design. The difficulty index (ranging from 0 to 1) represents the proportion of correct answers, with 0.5 indicating optimal difficulty. The discrimination index reflects a question’s ability to differentiate between high- and low-performing participants, with values ≥ 0.2 considered acceptable.
Phase II: practical skills performance evaluation. On the day following the training, all participants conducted a single ultrasound-guided interscalene brachial plexus block using in-plane technique on patients scheduled for shoulder or upper arm surgery under regional anesthesia combined with general anesthesia. Standard monitoring, oxygenation, and intravenous fluids were administered to each patient during the procedure. All trainees were allowed to proceed for a maximum of 30 min at the discretion of the supervisor (other than the expert evaluator), who was always present and intervened if (1) the patient became hemodynamically unstable, (2) the patient experienced paresthesia along the distribution of the brachial plexus, (3) if blood was noted on aspiration, or (4) if the procedure took longer than 30 min. Two onsite expert observers evaluated their performance using the 22-item procedural Checklist and a 9-item GRS [9]. The entire procedure took place in the operating theatre. The Checklist consisted of specific items that were graded either “0,” not performed; “1,” performed with prompting/ poorly performed; or “2,” unprompted and performed. The GRS consisted of a 5-point scale, with 9 items related to preparation, patient care, and technical skills specific to ultrasound-guided regional anesthesia (UGRA). The 22-item checklist measured task completion and procedural accuracy, while the GRS evaluated overall performance quality across key domains. The full instruments are provided in Appendix B.
Resource feedbackAfter the assessment, participants in VG were requested to complete a feedback questionnaire (see Appendix D for full details) independently, obtaining their opinions and feelings about the VR-assisted training program. The survey evaluated perceptions of the course’s difficulty level and inquired about its capacity to engage learners’ interest. Additionally, it gathered opinions on the program’s effectiveness in enabling participants to master nerve block procedures.
Statistical analysisThis pilot study focused on the feasibility of VR-based anatomy training for performing UGNB. The sample size, aimed at 10 participants per group, was chosen based on recommendations from the literature on medical education research [10] and not for statistical hypothesis testing.
The chi square and Fisher’s exact test was used to compare the distribution of gender, types of trainees. Normal distribution was observed for age, pretest and post-test results, and test scores gains in both groups. Independent t-tests were used to evaluate scoring differences between two groups regarding to score gains, GRS and the Checklist. Paired t-test was employed to assess disparities between pre-test and post-test scores. A Mann-Whitney U test was used to compare the differences of self-evaluation of the anatomy level and spatial ability between two groups. P < 0.05 indicated statistical significance. Statistical analysis was performed using SPSS Statistics Version 27.0 (IBM Corp, Armonk, NY).
留言 (0)