Study design and setting
The study was conducted at Wachemo University Nigist Elleni Mohammed Memorial Comprehensive Specialized Hospital. It is found in regions of southern nations, nationalities and peoples of Ethiopia. Nigest Elleni Mohammed Memorial Comprehensive Specialized Hospital (NEMMCH) is located in Hosanna town, Central Ethiopia region, Hadiya Zone. Hossana town is located 235 km and 181 km south of Addis Ababa city and from Hawassa city, respectively. Nigest Elleni Mohammed Memorial Comprehensive Specialized Hospital (NEMMCSH) is one of the oldest public hospitals in the country. It was established in 1975 G.C. Currently, it is a teaching and referral hospital in the central region of Ethiopia with a bed capacity of 350 beds that is managed by Wachemo University (WCU). Currently, many departments are running teaching and learning activities in hospitals. Teaching and referral hospitals provide services to nearly 3 million people in the catchment area, and approximately 450–500 patients visit hospitals each day. The hospital currently has 350 beds for patient and emergency activities. Similarly, it delivers 24-h emergency operative activities for general surgery and orthopedic procedures and delivers mothers with cesarean section in six separate theatres.
Study design and period
This was an observational study conducted from December 1, 2023, to June 30, 2024. All patients underwent surgery at Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital (NEMMCSH) from December 1, 2023, to June 30, 2024.
Source and study population
All adult patients aged 18 years and above who underwent both elective and emergency surgery at this study hospital composed the source population, whereas all adult patients aged 18 years and above who underwent surgery in this study area and fulfilled the inclusion criteria during the study period composed the study population.
Eligibility criteriaInclusion criteria
All adult fit and stable surgical patients who underwent surgery under anaesthesia in the postanaesthesia care unit during the study period were included in the study. Admission to the PACU was based on the federal Ministry of Health Ethiopia PACU protocol.
Exclusion criteria
Patients who were directly admitted to an ICU or ward after an operation.
Patients admitted to the PACU during the course of transfer to the ICU.
Pregnant patients and patients who experienced postoperative shivering were excluded from the study.
Patient with severe pain.
Patients with unstable vital signs while transferring from the operation theatre.
Patients who refused to give consent for inclusion in the study.
Sample size and sampling technique
The sample size was determined by using a single population proportion formula. A study performed in Ethiopia at the University of Gondar on the incidence of haemodynamic events in the postanaesthesia care unit reported that 59% of patients who underwent surgery had haemodynamic instability and was used to determine the sample size of this study [1].
The sample size for this study was calculated by considering the 95% confidence interval, 5% margin of error, and 59% proportion. Population correction was used since the source population was < 10,000. Situational analysis of surgical patients was performed 3 months before the start of the study, and an average of 360 procedures were performed per month.
The sample size was calculated as follows.
$$\frac^ 0.59\left(0.41\right)}^}$$
where n: sample size p: proportion d: absolute precision.
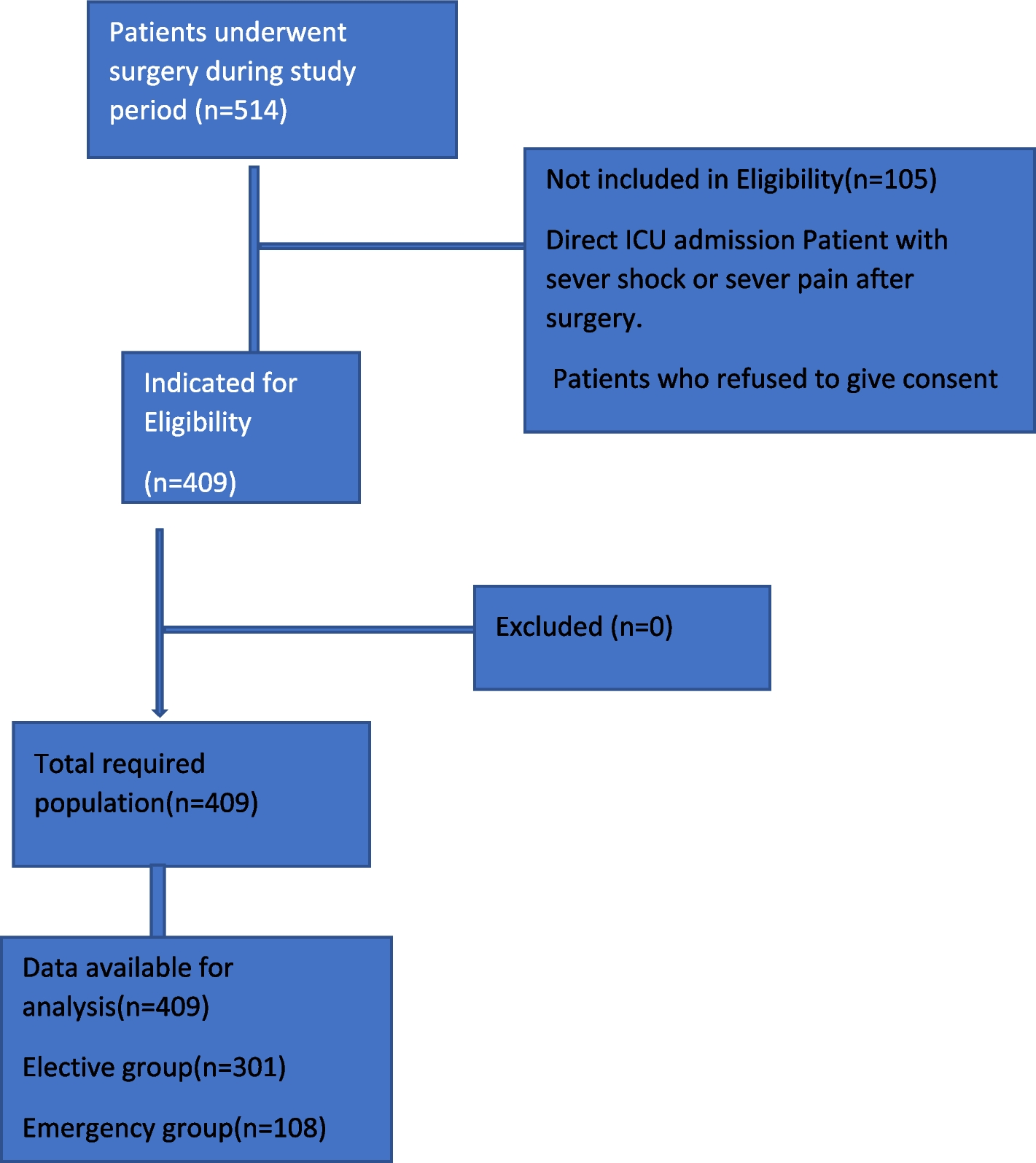
When a 10% nonresponse rate was added, the total number of patients included in the study was 409.
Sampling technique
We used a systematic random sampling technique to select the appropriate participant in a sample at a regular interval is selected on the basis of the sampling fraction (K). K = sampling interval, N = total study population and n = sample number.
According to the hospital analysis, 1080 surgical patients were treated within three months.
N = 360, n = 409
K = N/n………..1080/409 = 2.9≈3, the sampling fraction was three, and the first participant was taken by using the lottery method for daily elective patients.
Study variablesDependent variables
Postoperative hemodynamic changes (HR, BP).
Independent variables
Anaesthesia-related variables
Anaesthesia drugs used
Fluid management strategies
Procedure-related variables
Blood loss during surgery
Duration of surgery
Operational definitionsHemodynamic instability
If a patient has at least one physiological parameter that changes from baseline, including systemic hypertension, hypotension, tachycardia, or bradycardia alone or in combination, then the patient has experienced hemodynamic instability [1, 18].
1.
Baseline values were measured before induction [19].
2.
Hypotension: a decrease in mean arterial pressure by 20% from the baseline mean arterial pressure or MAP < 60 mmHg and SAP < 90 mmHg [13, 20].
3.
Hypertensive: an increase in mean arterial pressure of 20% from the baseline mean arterial pressure or SAP ≥ 140 mmHg [13, 14].
4.
Tachycardia: Heart rate ≥ 100 for adults [10, 21].
5.
Bradycardia: Heart rate ≤ 60 for adults [10, 21]
Data collection tools, methods and procedures
A questionnaire was developed after carefully reviewing different literature (Supplementary file), and data were collected by two anaesthetists and three nurses. A chart review was used to collect the data. The questionnaire was prepared to address the preoperative data of patients, such as age, sex, BMI, NPO hour, history of medical illness, and history of medication usage. Blood pressure, heart rate, temperature, and oxygen saturation were recorded during the intraoperative period. Anaesthetic and surgical variables such as the urgency of surgery, duration of surgery, type of anaesthesia, intraoperative estimated blood loss, timing of surgery, intraoperative fluid administered, and intraoperative haemodynamic instability were recorded in the questionnaire. The patient’s hemodynamic status assessment started within the first 15 min of arrival at the PACU.
Data on hemodynamic variables (HR, BP) were collected every 15 min during the first 1 h of the PACU stay and every 30 min during the second hour of the PACU stay as per PACU monitoring standards [20].
Preoperative fasting protocol (Table
1)
Table 1 ASA fasting protocolData quality assurance
To ensure the quality of the data, training on the objectives and relevance of the study and brief orientations on the assessment tools were provided for the data collectors. The questionnaires were prepared in English and pretested on 5% of the study population. The Cronbach’s alpha of the pretest was 0.87. During data collection, each question was revised by the investigator to be complete and appropriate. In the event of missed measurements during the intraoperative period, the electronic data stored by the monitoring equipment were recalled and backtraced, and the data were filled.
Data analysis
Epi Data version 4.6 was used to code, edit, clear and enter the data. The data were then exported to the Statistical Package for Social Sciences (SPSS) software version 26 for further analysis. For both ordinal and nominal categorical variables, a stack bar was used to show the distribution of categorical variables, and nominal logistic regression was used for both ordinal and nominal categorical variables. Socio-demographic and related characteristics of the patients and anaesthetic and surgical-related variables were analysed and presented in texts, tables and graphs.
The normality of the distribution of the data was tested via the Shapiro‒Wilk test. Normally distributed data are presented as means and standard deviations, whereas nonnormally distributed data are presented as medians or interquartile ranges. The crude odds ratio (COR) and adjusted odds ratio (AOR) with the corresponding 95% confidence interval were calculated to determine the strength of the factors associated with hemodynamic instability. Model fitness was checked via the Hosmer–Lemeshow test.
Both bivariable and multivariable logistic regression analyses were performed to assess the associations between the dependent and independent variables. Independent variables with p < 0.2 at the 95% CI in the bivariable analysis were transferred to the multivariable binary logistic regression analysis. In multivariable regression, variables with p values < 0.05 were considered statistically significant predictive factors for haemodynamic instability in the postanaesthesia care unit.




留言 (0)