
記住我


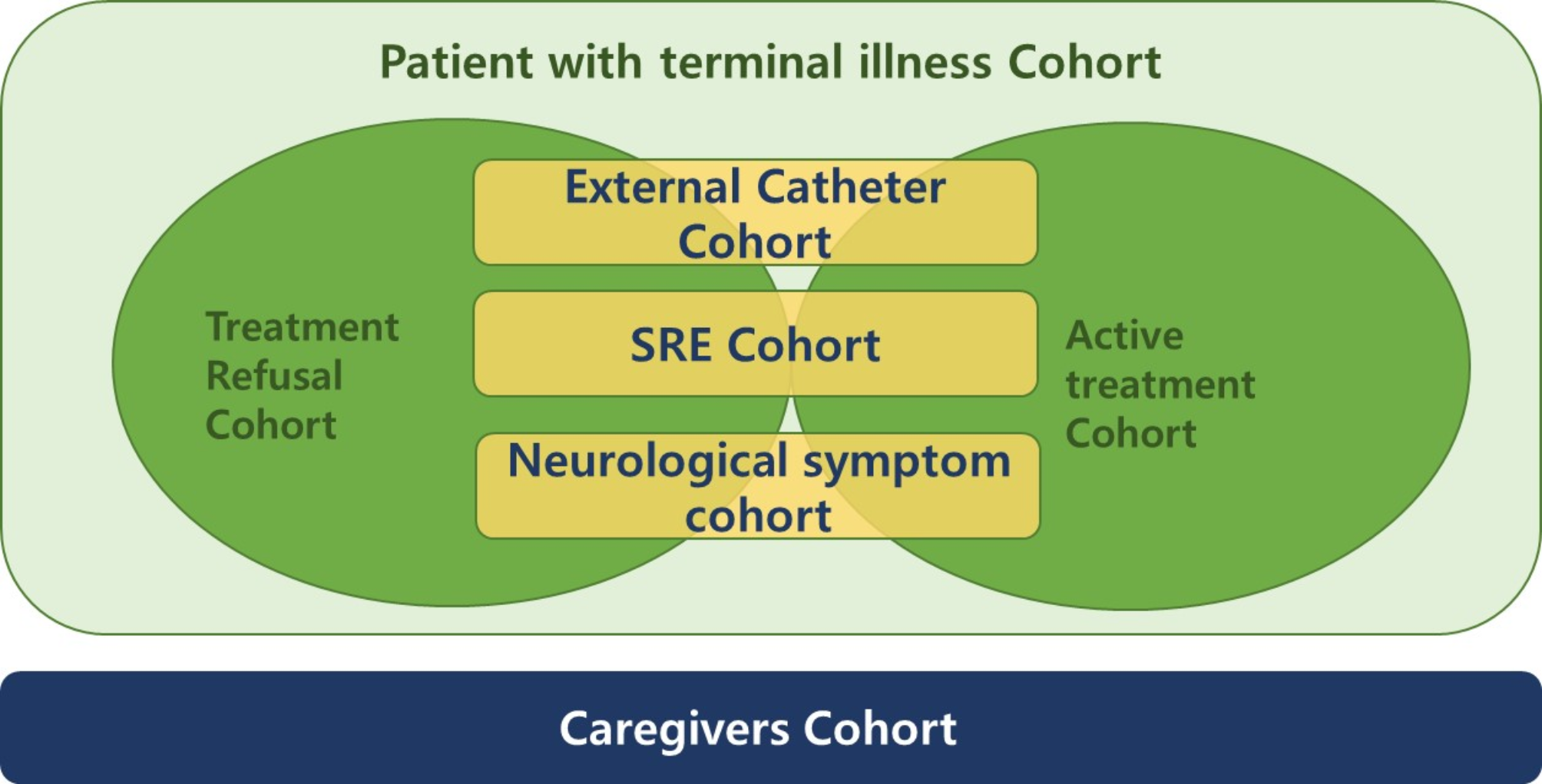

This study aims to evaluate the quality of life of patients with advanced cancer, and their caregivers, who visit regional cancer centers throughout their disease trajectory, to contribute to this understanding. This multicenter prospective observational cohort study utilizes a comprehensive approach, consisting of two cohorts and five sub-cohorts. The aim is to explore the changes in the quality of life of patients (and caregivers) who are relatively more burdened by their disease and are likely to be socially isolated throughout the disease trajectory. Ten hospitals in a regional cancer center and two affiliated hospitals have joined the study. Through consensus, investigators have identified several clinical characteristics that are likely to impact the quality of life of patients with advanced cancer who visit regional cancer centers. These include patients who have declined active cancer treatment regardless of cancer stage (treatment refusal cohort), those with external catheters (external catheter cohort), those with primary or secondary brain tumors or neurological symptoms from spinal metastasis (neurological symptom cohort), and those with skeletal-related events (SRE) cohort (Fig. 1). SREs are defined as pathological fractures, paralysis, spinal cord compression, bone pain, or impending fractures requiring radiation therapy or surgery.
Fig. 1
Diagram of cohorts and sub-cohorts of the study
Primary aims 1.To examine changes in quality of life over the last year of life (at 3, 6, 9, and 12 months).
2.To assess depression and anxiety levels over the last year of life (at 3, 6, 9, and 12 months).
3.To evaluate pain intensity over the last year of life (at 3, 6, 9, and 12 months).
Secondary aims 1.Survival time, quality of life, and complications following external catheter insertion procedures.
2.Survival time, quality of life, and related factors in patients who did not receive active treatment.
3.Quality of life in patients with spinal metastases, brain metastases, and neurological symptoms.
4.Quality of life in patients with skeletal-related events (SREs).
5.Transfer status, treatment modalities, and outcomes of patients transferred from other hospitals.
6.Hospice utilization rate, hospice death, and length of stay.
7.Emergency department and intensive care unit utilization at 1, 3, 6, 9, and 12 months before death.
8.Hospitalization rate, reasons for hospitalization, and deaths at 1, 3, 6, 9, and 12 months before death.
9.Types, completion rates, and decision makers of end-of-life care-related documents for terminal patients.
10.Confirmation of active cancer treatment within 1, 3, and 6 months before death 1-month mortality rate of cancer patients using the emergency department.
11.Quality of life and bereavement of caregivers due to caregiving burden.
Inclusion criteriaCommon criteria for patientsCommon criteria include patients who are aged 19 or older and who have cancer (solid or hematologic) for which a cure is not expected at the time of enrollment.
For the treatment refusal cohort, enrollment is possible regardless of stage.
Written informed consent was obtained from all the patients.
Criteria for patient sub-cohorts① Treatment refusal cohort: Cancer patients who have refused anticancer, surgical, or radiation therapy for treatment purposes, regardless of stage.
② External catheter cohort: Cancer patients who have external catheters or who have been transferred with external catheters (urinary catheters and vascular catheters are excluded).
③ Neurological symptom cohort: Patients with primary or secondary brain metastasis or spinal metastasis with neurological symptoms.
④ SRE cohort: patients with SREs (SREs are defined as pathological fractures, paralysis, spinal cord compression, pain, or impending fractures requiring radiation therapy or surgery).
Patients who meet the criteria for two or more cohorts can be enrolled multiple times.
Criteria for caregiversInclusion criteria include caregivers of enrolled patients, who are aged 19 or older, and who accompany the patient to medical appointments, primarily provide care, or are actively involved in the patient’s treatment decisions.
Exclusion criteriaPatients whose cancer has not been histologically confirmed are excluded from the study.
Sample size calculationThe total sample size of this study is 720 patients from ten hospitals. This number is based on the testing of the primary outcome, which is the degree of change in the continuously measured Numerical Rating Scale (NRS) scores for one year. The sample size is determined using a longitudinal (repeated measures) cluster prospective cohort study design.
To calculate the required number of patients for one hospital, the change in the NRS score is assumed to be 5.5-point based on a previous study that measured a change from 6.5 to 1.0 in NRS scores among palliative care patients [13]. The minimal clinically important difference (MCID)—the smallest change in the clinical outcome that a patient would consider meaningful—is assumed to be 4.0, based on consensus among the participating researchers. The agreement at each measurement point at which the NRS is scheduled to be measured four times is assumed to be 0.6. The Type I error (α), Type II error (β), and dropout rate are set at 0.05, 0.20, and 10%, respectively. When we apply the equation (Supplementary 1) to the longitudinal cluster prospective cohort study [14], the number is 24 patients. Since this study involves ten hospitals over one year, the total sample size of patients is 240 (or 720 over three years).
However, because the number of patients available for treatment at each participating hospital varies, weights are applied to the required number of patients at each hospital based on the number of patients treated over the previous three years. The weights are listed in Supplementary 2.
Statistical analysisThe mean (± SD) is presented for continuous variables when the data meets the assumptions of normal distribution and homoscedasticity. To check these assumptions, the Shapiro-Wilk test is used for normality, and Levene’s test is used for homoscedasticity. If either assumption is violated, the median (interquartile range) is presented instead. Categorical variables are presented as frequencies and percentages (N %).
The baseline characteristics of the enrolled patients, including age, sex, cancer type, stage, ECOG performance status, Charlson Comorbidity index, treatments, hospital information, and outcomes (e.g., EQ-5D-5 L, the Hospital Anxiety and Depression Scale (HADS), Edmonton symptoms assessment scale (ESAS [15]) score, Krean-Modified Barthel Index (K-MBI [16]), and Korean version of Memorial Delirium Assessment Scale (K-MDAS [17])), Korean-Mental State Examination2 (K-MMSE [18]) are presented. Outcomes are measured at three-month intervals. These are described and plotted. Generalized estimating equation (GEE) analysis is performed to assess the changes in these outcomes over time.
The characteristics of patients with and without catheter therapy are compared using standardized differences, with values greater than 0.2 indicating meaningful differences. The difference in 1-year mortality between the two groups is evaluated using survival analysis. Subsequently, multivariate Cox proportional regression analysis is used to calculate the hazard ratio (HR) for the catheter insertion group after adjusting for significant patient characteristics. These analyses are conducted to compare patients with and without brain metastases, those transferred from other hospitals, those receiving systemic chemotherapy, and those visiting the emergency room.
The Cochran Q test is conducted to assess changes in hospice utilization, emergency room visits, intensive care unit admissions, hospitalization rates, and reasons for hospitalization at one, three, six, nine, and twelve months before death. All statistical analyses are performed using the R 4.3.2 (Vienna, Austria).
Recruitment and data collectionThis study protocol and study-related documents, including an informed consent form, an electronic case recording form, and questionnaires, have been approved by each participating hospital. This study was registered at https://cris.nih.go.kr(KCT0009177) on February 16, 2024. Patients and their caregivers who meet the inclusion and exclusion criteria will be enrolled in the study for three years.
Baseline clinical characteristics, comorbidities, cancer diagnosis, cancer treatment, socioeconomic status, and healthcare system utilization data of patients will be collected at the time of registration. The caregivers’ demographic data, relationships with patients, jobs, and religion will be collected at the time of registration.
Clinical information and patient-reported outcomes (PROMs) will be collected every three months until death or the end of the study. The caregiver will respond to the PROMs every three months after the patient dies for one year. The allowable window period for a 3-month visit is one month. Anti-cancer treatments, medical utilities (Intensive care unit care, emergency room visit, hospitalization, or hospice care), ECOG performance status, co-morbidities, laboratory work (CBC, chemistry), and writing advance directives will be collected for each visit. The patients and caregivers will be asked to complete a quality-of-life questionnaire at each visit. These include: the HADS, Nutritional Risk Screening 2002, ESAS, and EQ-5D-5 L. The caregivers will complete the HADS and the Korean version of the Caregiver Quality of Life Index-cancer [19] at each visit. After the patient’s death, the caregivers’ questionnaires will include the Good Death Inventory [20].
The patients with neurological symptoms and SRE cohorts will have an additional one-month follow-up with a 15-day window. The K-MBI, K-MDAS, and Korean-Mental State Examination2 will be applied for those cohorts.
A schedule for collecting information and implementing PROMs are provided (Tabel 1 and Table 2).
Table 1 Cohort follow-up schedule for patientsTable 2 Cohort follow-up schedule for caregiversThis study is part of the KOREAN CANCER SURVIVOR HEALTHCARE R&D PROJECT (KOCAS) and will be conducted using the data collection e-CRF and an electronic survey system in the cloud system provided by KOCAS. The data will be anonymized and made publicly available in the system after the completion of the study.
Ethical statementThe current study will comply with ethical standards presented in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The study protocol was approved by the institutional review boards at Kangwon National University Hospital (KNUH 2023-10-003), Gyeongsang National University Hospital (GNUH 2023-07-012), Gachon University Gil Medical Center (GBIRB2023-277), Pusan National University Hospital (2307-008-129), Chungnam National University Sejong Hospital (CNUSH 2023-05-010), Ajou University Hospital (AJOUIRB-OB-2023-330), Ulsan University Hospital (UUH2023-06-022), Jeonbuk National University Hospital (CUH IRB 2023-11-026), Jeju National University Hospital (JEJUNUH 2023-08-006), Gyeongsang National University Changwon Hospital (GNUCH 2024-05-018), Chungbuk National University Hospital (CBNUH 2023-06-029), Chungnam National University Hospital (CNUH 2023-09-023) and registered with cris.nih.go.kr (KCT0009177); research nurses and investigators will screen and explain the aim and procedure of the study to the participants (patients with cancer and their caregivers) and will obtain the informed consent.
留言 (0)