
記住我



The training set comprised 501 patients with an average age of 48.63 (9.41) years, while the validation set consisted of 1,533 patients with an average age of 49.01 (9.51) years. Among them, 1,097 patients (53.9%) were menopause, and 179 patients (8.8%) had a family history. A total of 1,063 patients (52.3%) were classified as TNM stage II, and 998 patients (49.1%) were classified as TNM stage III. There were no significant differences in all pathological parameters between the two groups of patients (all P > 0.05), as shown in Table 1.
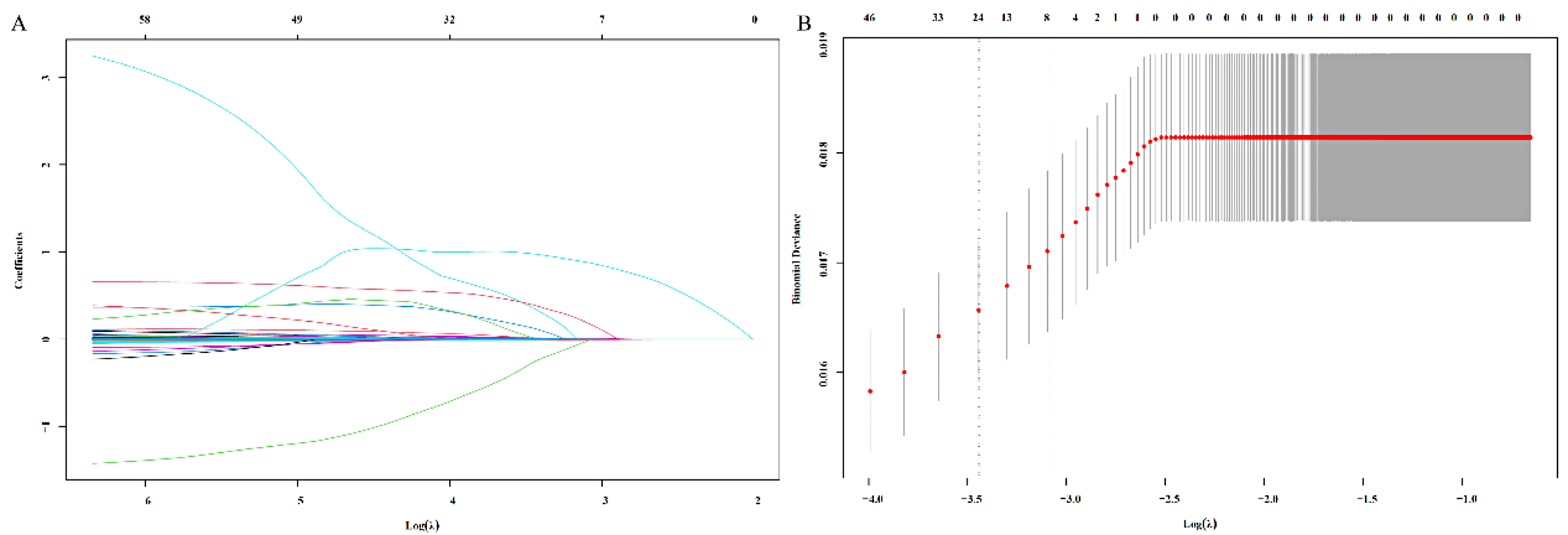
Table 1 Patients’ characteristicsConstruction of risk indexAll blood parameters were included in the Lasso regression model for analysis, with the regularization strength λ systematically adjusted to optimize variable selection (Fig. 1A, B). As λ increased, less significant parameters were excluded, leaving only the most predictive factors. When λ = 0.001, only ALB and NLR remained significant, indicating their strong contribution to the model. Based on the Lasso regression coefficients, the ANLR index was constructed as follows: ANLR index = NLR − 0.04 × ALB (g/L).
Fig. 1
Establishment of the Lasso model (A) and calculation of the optimal λ value (B)
The prognostic value of ANLR indexThe ANLR index achieved a maximum Youden index of approximately 0.247 when calculated using an ROC curve focused on mortality, with an optimal cutoff value of 1.05 (Fig. 2).
Fig. 2
Furthermore, compared with other classical inflammatory markers, ANLR exhibited the highest AUC of 0.694 (Table 2).
Table 2 The AUC of ANLR and classical inflammatory markersSurvival analysis of ANLR indexSurvival analysis in training setThe timeROC analysis for ANLR showed that the 3-, 4-, and 5-year AUCs for DFS were 0.657, 0.713, and 0.692, and for OS were 0.643, 0.707, and 0.679, respectively (Fig. 3A, B). Patients with higher ANLR had significantly shorter DFS (408 cases vs. 93 cases, χ2 = 3.735, P < 0.001) and OS (408 cases vs. 93 cases, χ2 = 4.117, P < 0.001, Fig. 3C, D).
Fig. 3
Survival analysis in Training set. (A) The timeROC of ANLR in DFS; (B) The timeROC of ANLR in OS; (C) The survival curve of ANLR in DFS; (D) The survival curve of ANLR in OS
Survival analysis in test setIn the validation set, timeROC analysis for ANLR revealed 3-, 4-, and 5-year AUCs of 0.696, 0.717, and 0.693 for DFS, and 0.684, 0.719, and 0.692 for OS (Fig. 4A, B). Patients with higher ANLR values exhibited significantly shorter DFS and OS (1239 cases vs. 294 cases, χ2 = 3.889, P < 0.001 and χ2 = 4.746, P < 0.001, Fig. 4C, D). The risk analysis of ANLR index also revealed significant differences between high-risk and low-risk groups (Fig. 4E, F).
Fig. 4
Survival analysis in Test set. (A) The timeROC of ANLR in DFS; (B) The timeROC of ANLR in OS; (C) The survival curve of ANLR in DFS; (D) The survival curve of ANLR in OS; (E) The risk analysis of ANLR in DFS; (F) The risk analysis of ANLR in OS
Cox survival analysisIn the validation set, univariate analysis revealed that tumor size, lymph node positivity (LNP), histological grading, TNM stage, and ANLR index were all associated with DFS and OS (all P < 0.05). Further multivariate analysis identified LNP (HR = 1.544, P < 0.001 and HR = 1.995, P < 0.001), TNM stage (HR = 2.582, P < 0.001 and HR = 2.796, P < 0.001) and ANLR (HR = 3.551, P < 0.001 and HR = 3.798, P < 0.001) as independent prognostic factors for both DFS and OS (Tables 3 and 4).
Table 3 Univariate Cox analysis of DFS and OSTable 4 Multivariate Cox analysis of DFS and OSPropensity score matching analysis for ANLRIn the validation set, correlation analysis showed that the ANLR index was significantly associated with age, BMI, family history, PLN, tumor size, histological grading, and TNM stage (all P < 0.05). Based on these correlation analysis results, we selected variables with significant statistical associations for PSM. A 1:1 nearest-neighbor matching method without replacement was applied to ensure that patients with similar prognostic characteristics were paired. Through this matching process, a total of 152 patients were included, with 76 in the high ANLR group and 76 in the low ANLR group. After matching, there were no significant differences in baseline clinical characteristics between the two ANLR groups (all P > 0.05, Table 5), confirming the balance and comparability of the matched cohorts. This rigorous matching process ensures that the observed prognostic differences are primarily attributable to the ANLR index.
Table 5 Propensity score matching analysisAfter PSM, the 3-, 4-, and 5-year AUCs for DFS of ANLR were 0.647, 0.672, and 0.666, respectively, and for OS were 0.668, 0.655, and 0.653, respectively (Fig. 5A, B). Higher ANLR remained associated with shorter DFS and OS (76 cases vs. 76 cases, χ2 = 2.179, P = 0.001 and χ2 = 2.063, P = 0.002, Fig. 5C, D).
Fig. 5
Survival analysis after PSM. (A) The timeROC of ANLR in DFS; (B) The timeROC of ANLR in OS; (C) The survival curve of ANLR in DFS; (D) The survival curve of ANLR in OS
Comparison of prognostic value of ANLR in different periodsBy collecting the levels of ALB, NEU, and LYM the day before surgery, the preoperative ANLR index (pANLR) was calculated. The timeROC curve analysis showed that the AUC of ANLR for both DFS and OS was higher than that of pANLR at all stages (Fig. 6).
Fig. 6
The timeROC curve of ANLR and pANLR
Construction of nomogramsThe Schoenfeld residual plots indicated that both TNM stage and the ANLR index met the proportional hazards assumption (all P > 0.05, Fig. 7A, B). The nomograms incorporating TNM stage and the ANLR index were developed in the training set (Fig. 7C, D). The C-index for the nomogram in the training set was 0.742 (0.619–0.886) for DFS and 0.758 (0.607–0.821) for OS, while in the validation set, the C-index was 0.733 (0.655–0.791) for DFS and 0.714 (0.634-0.800) for OS. Calibration curves based on the validation set demonstrated good agreement of the nomogram (Fig. 7E, F).
Fig. 7
Construction of nomograms. (A) Schoenfeld residual plots of DFS; (B) Schoenfeld residual plots of OS; (C) Nomogram of DFS; (D) Nomogram of OS; (E Calibration curve of DFS; (F) Calibration curve of OS
留言 (0)