
記住我

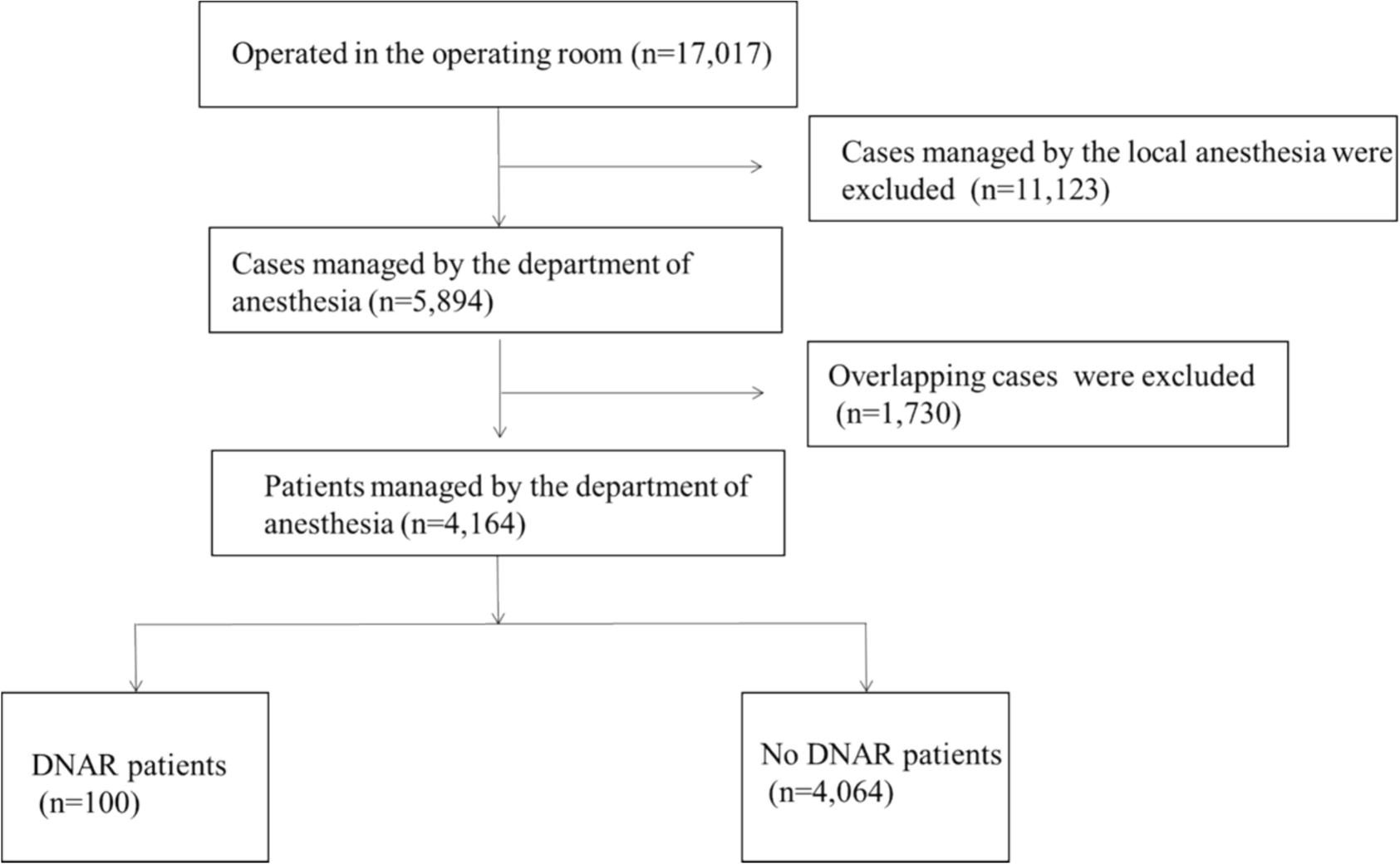
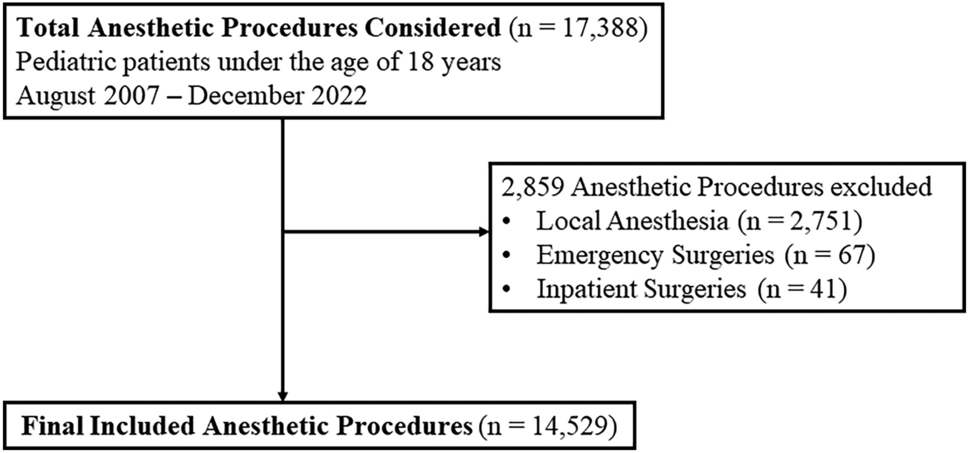
Between August 2007 and December 2022, 14,529 anesthetic procedures for day surgery in 11,818 patients were performed. Twenty-eight (0.19%) of 14,529 anesthetic procedures at our hospital during the study period required UHA. Figure 1 illustrates the inclusion and exclusion process for anesthetic procedures in this study. Table 1 summarizes the characteristics of the 14,529 anesthetic procedures for whom complete data were available. Patients who required UHA were older than those who did not (age group 12–17 years; 18% vs. 4.0%, P = 0.045) and were more likely to have a higher ASA-PS score (score > 2; 3.6% vs. 0.11%, P = 0.036). Patients who required UHA also underwent more urologic procedures (43% vs. 18%, P = 0.017) and were more likely to have surgeries lasting >2 h (3.6% vs. 0.19%, P < 0.001) and to exit the operating room after 15:00 (18% vs. 0.34%, P < 0.001).
Fig. 1 Table 1 Characteristics of 14,529 patients according to UHA statusReasons for UHA
Table 1 Characteristics of 14,529 patients according to UHA statusReasons for UHATwenty-four (86%) of the 28 patients with UHA required inpatient admission before their initial discharge and 4 (14%) required inpatient admission following a visit to the emergency department within 24 h of day surgery. The most common reasons for UHA were anesthesia-related, the most frequent being PONV, which occurred in 10 patients (36%), and required a mean hospital stay of 2 days (Table 2). Newly identified medical conditions (hypoglycemia, seizure, ascites, gastroenteritis) accounted for 4 UHA (14%) and required the longest average hospital stay at 22 days. Surgical complications led to 6 UHA (22%) that required a mean hospital stay of 2 days (Table 2).
Table 2 Reasons for unplanned hospital admissions (n = 28)Among the anesthetic-related admissions, intravenous fluids were the most common intervention (n = 10, 36%), followed by antiemetic treatment with medications such as dexamethasone, metoclopramide, and famotidine (n = 6, 21%). Analgesic medications were provided in 2 cases (7.1%), including acetaminophen, nonsteroidal anti-inflammatory drugs, and fentanyl.
For medical-related admissions, nonsurgical interventions were predominant (n = 6), including intravenous fluids, intensive care for seizures and hypoglycemia, seizure treatment, diuretic therapy for ascites, and inhalation treatment for asthma. Surgical intervention was required in 1 case (3.6%), where endoscopic examination revealed ascites, leading to a diagnosis of Wilms tumor and tumor resection. One other patient (3.6%) was managed with observation only for a high fever. Intravenous line insertion was not feasible, and the patient was supported through breastfeeding (Table 3).
Table 3 Interventions provided for unplanned hospital admissions according to reason (n = 28)In the surgical category, all 6 patients (18%) required surgical intervention to address the complications, including 2 cases of hemostatic surgery for bleeding, abscess drainage for infection, revision surgery for rectovaginal fistula found after vaginoplasty, surgery for a suspected polyp that was found to be hemorrhoids requiring hemorrhoidectomy, and a planned inguinal hernia repair where a suspected cancer was found near the testicle. One patient (3.6%) also received nonsurgical intervention with antibiotic therapy for a surgical site infection.
In the social category, observation without specific medical or surgical intervention was undertaken for 3 patients (11%). Eight children in the hospital admission group received more than one type of intervention.
Subsequent hospital courseTwenty-four (86%) of the 28 patients who experienced UHA were discharged after a hospital stay of 1–2 days. The remaining 4 patients (14%) experienced more extended admissions that ranged from 6 to 182 days. Two patients experienced postoperative infections and recovered after appropriate treatment. One patient returned to the emergency department with fever, diarrhea, and vomiting after inguinal hernia repair and was diagnosed with infectious gastroenteritis. This patient received intravenous fluids and was discharged after a 7-day hospital stay. Another patient developed a postoperative wound infection after inguinal hernia repair, presenting with fever. The infection required incision and drainage, followed by intravenous antibiotic therapy, and the patient was discharged after a 6-day hospital stay. The third patient was hospitalized for a prolonged period after an incidental diagnosis of Wilms tumor during admission for an unrelated condition. This patient underwent surgical resection of the tumor followed by chemoradiotherapy, with a total hospital stay of 182 days. The patient passed away 3 months after discharge due to progression of the underlying cancer. One patient experienced a severe postoperative course, with complications likely associated with critical hypoglycemia, and died during the follow-up period.
Risk factors for UHAThe results of the multivariable logistic regression analysis of the first anesthetic procedures in 11,818 patients during the study period are summarized in Table 4. The incidence of the UHA was 27 (0.23%). The risk of UHA was significantly higher in patients who exited the operating room after 15:00 than in those who exited between 09:00 and 11:59 (adjusted Odds ratio 29.3; 95% CI [7.09, 121]; P < 0.001). Longer operation time was also associated with a higher risk of UHA (adjusted Odds ratio 1.03; 95% CI [1.01, 1.04]; P < 0.001).
Table 4 Risk factors associated with unplanned hospital admission identified by multivariable logistic regression analysis (n = 14,529)Subgroup analysisThe median (IQR) operation time for the UHA group was significantly longer than that for the non-UHA group, at 106 (72, 112) min versus 15 (6, 36) min, respectively (P = 0.0057). This result supports the finding that surgery duration independently contributes to UHA risk and further validates the multivariable logistic regression analysis in Table 4.
留言 (0)