DMD can be thought of as a serious condition with unmet need, criteria that qualify new therapies for accelerated regulatory approval [17]. Accelerated pathways aim to foster therapeutic innovation by expediting the availability of new drugs for rare diseases. However, this positive goal has inadvertently fostered pathways that allow new DMD drugs to achieve regulatory approval prematurely. We examine these ideas in the sections that follow.
3.1 SSHY Studies and the Accelerated Regulatory Pathway
The acronym ‘SSHY’ describes characteristics of the studies that allow new DMD drugs to qualify for accelerated regulatory approval: short (duration), small (size of study population), healthy (baseline medical status of subjects), and/or young (subjects’ age). Regarding our definitions, as discussed below, the clinical course of DMD typically extends into the third decade of life and beyond, with the most impactful cardiorespiratory complications occurring in "older," non-ambulatory individuals. In terms of this clinical context, we describe the ambulatory populations in the listed studies as "healthy" and "young," and the time intervals studied as "short."
In Table 1, we show all the new DMD drugs provisionally approved by the US FDA under the accelerated pathway and the SSHY characteristics of the studies on which the approvals are based. (The Table is current through July 1, 2024; additional details on recent approvals of the drug ELEVIDYS appear in Sect. 4.2.) The data used by FDA for each drug’s approval are shown. There is no central repository of this information; the sources are presented in the reference list [20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50]
Table 1 SSHY characteristics of studies of drugs for Duchenne muscular dystrophy approved under the US Food and Drug Administration (FDA) accelerated regulatory pathway (current to July 1, 2024).Of note, Table 1 includes almost all the therapies for DMD currently approved by the FDA under both accelerated and traditional pathways. For a continuously updated list, see https://www.parentprojectmd.org/duchenne-drug-development-pipeline/. The therapies that would complete the list are: deflazacort, one of the GCs that, like prednisone, is a part of DMD standard of care (SOC), and givinostat, a histone deacetylase inhibitor that was recently granted full FDA approval, whose aim is to decrease muscle damage due to inflammation, regeneration, and resulting fibrosis.
SSHY studies are faster and less costly to perform than traditional studies that require recruitment of larger populations and longer periods of follow-up. Their short duration means that study results can be generated quickly. However, SSHY studies have critical limitations. They cannot demonstrate long-term benefits; they focus on young, ambulatory populations; and they primarily assess functional motor strength, with outcomes such as rise and walk tests and the North Star Ambulatory Assessment scale. The clinical implication of these functional outcomes is uncertain—the results can be used, for example, to predict subsequent loss of ambulation (LOA) [51], but their correlation with systemic morbidities and with mortality is unproven. By contrast, cardiorespiratory dysfunction is the unequivocal cause of DMD’s most significant clinical morbidities and is associated with shortened survival. These include acute respiratory events, such as pneumonia and mucus plugging due to ineffective coughing, and chronic complications, such as the need for mechanically assisted ventilation via mask or tracheostomy. From a cardiac point of view, morbidities include acute and chronic presentations of cardiomyopathy—complications that can lead to heart failure and premature death. Cardiorespiratory complications like these essentially never occur in the young, ambulatory individuals comprising the population of current drug studies; instead, they affect older individuals who are in the late, non-ambulatory stage of DMD [1, 4, 5, 52,53,54]. Moreover, when patients are treated with assisted ventilation to compensate for their chronic respiratory failure, cardiac function is the main determinant of their survival [54], yet a review of Table 1 reveals a complete absence of cardiac data.
Despite these limitations, under the accelerated pathway, results from SSHY studies suffice for provisional regulatory approval of new DMD drugs and their use on patients. Additionally, as shown in Table 1, regulators place a heavy emphasis on surrogate outcomes, especially the ability of a drug to increase tissue levels of non-biologic, truncated dystrophin protein. However, this surrogate outcome measure is controversial, in part because various aspects of its clinical effects—including minimum threshold levels of effectiveness, dose–response, and association with muscle strength scales—are unknown and/or unproven [36, 42, 43].
Although full regulatory approval is predicated on positive results from larger, better-designed confirmatory studies, those studies are often delayed by years, and no confirmatory studies have been completed involving any of the drugs in Table 1. Revocation of provisional approval by FDA is rare, even for drugs that have ultimately been found to be ineffective, have caused severe side effects, or have failed, in real-world experience, to replicate the results of the pilot studies that led to their approval [10, 55,56,57,58,59].
In the next sections of this article, we focus on the respiratory outcome measures employed in current DMD drug studies. When those outcomes are suboptimal, drug efficacy cannot be accurately assessed.
3.2 The Limitations of Threshold Pulmonary Function Values
The first respiratory methodology that we discuss is the ability of a drug to delay the age at which individuals reach certain levels of pulmonary function. It has become common practice for studies to claim that a drug has respiratory benefits if it delays an individual’s decline to an FVC level of 60% predicted; an FVC of 50%; an FVC of 30% predicted; and/or an FVC of 1 liter[60,61,62,63,64,65,66]. In the case of the percent predicted FVC values listed above, these are the levels at which various respiratory treatments are recommended in the DMD care guidelines, including those published in 2018 [4] (i.e., lung volume recruitment at FVC ≤ 60% predicted; assisted coughing and ventilation at < 50% predicted) and in 2010 (ventilation at FVC < 30% predicted) [67]. These threshold levels were based solely on expert opinion to encourage anticipatory initiation of assisted ventilation. The thresholds are clinical strategies—they were not intended as outcome measures and have never been clinically validated (in one report, FVC < 50% predicted was actually a poor predictor of nocturnal hypoventilation [68]). For example, no one knows whether initiating assisted ventilation exactly when FVC falls below 50% predicted results in better patient outcomes, such as delaying or preventing pneumonia, atelectasis, and/or hospitalizations, or whether this strategy prolongs lifespan. Similarly, a delay in time to reach FVC < 1 liter is the basis of inaccurate claims that a drug will prolong survival. In a seminal study published in 2001, a fall in FVC to a level < 1 liter was an ominous sign, with subsequent mean survival of 3.1 years, and 5-year survival of just 8% [69]. However, that was a natural history study, and the patients were not treated with current SOC. With assisted ventilation, patients with DMD can experience prolonged survival at any FVC level, even when their FVC is unmeasurably low and they require continuous ventilatory support [6]. Thus, the claim that delaying FVC decline to < 1 liter prolongs survival is inaccurate and ignores the benefits of assisted ventilation [4, 6, 54].
3.3 Concerns Regarding the Use of Historical Control Databases
Current studies of new DMD drugs use historical controls as their comparison group. The rationale is that DMD is a rare disease, making randomized trials difficult to perform. Currently, historical controls are derived from the databases of just a few academic consortiums [70, 71].
However, results from historical databases are quite variable, allowing drug studies to choose the most pessimistic controls for judging a drug’s efficacy. Faster rates of pulmonary function decline in the control group make it easier to show that a new drug is beneficial by lowering the bar that the study drug must exceed to appear effective.
For example, in a recently published study of the monoclonal antibody pamrevlumab for the treatment of DMD [72], three different historical control databases were compared with the study drug. With the drug, FVC %pred declined 4.0% after 1 year of therapy. The databases discussed as potential controls varied in their rate of decline from 5.5 to 8.7% per year. No statistical significance was reported when the drug was compared with the Cooperative International Neuromuscular Research Group (CINRG); however, the drug was reported to have a statistically significant benefit when compared with a more pessimistic database, the phase III DELOS (Study of Idebenone in Duchenne Muscular Dystrophy) [72, 73]. Subjects who received pamrevlumab were also treated with a “stable dose” of GCs, and GCs are known to mitigate decline in pulmonary function in individuals with DMD [64]. However, GC “dosages and schedules were not available” for one of the historical control groups (CINRG); and the historical control group chosen for the comparator (DELOS) was not receiving GC therapy [72, 73]. This example illustrates how studies of new drugs can pick and choose pessimistic historical control data that make it easier to demonstrate a beneficial drug effect. It also illustrates that comparability in key variables—in this case, GC therapy—can be lacking [72]. In the pamrevlumab study, the better pulmonary function displayed by the treated group could have been due to GC treatment and not the positive effects of the drug. This type of error reflects the observational nature of historical databases. When data are acquired prospectively, the nature and quality of relevant variables are known. Historical databases lack this rigor because of their observational nature [64]. Their outcome data embody treatment by many different clinicians, pulmonary function testing by different technicians, and variations in institutional treatment protocols. Thus, their results are subject to the influence of numerous uncontrolled variables, with unpredictable effects. Indeed, variability in clinical management is a hallmark of historical databases. Numerous studies have examined real-world enactment of SOC, including GCs [64]. They have found that adherence to the standards is low, implementation varies between centers, and the reasons for poor implementation are complex [74,75,76,77,78]. Consistent with these findings, databases currently used as historical controls fail to report crucial details on variability in GC formulations, doses, and schedules; relevant treatment changes and pauses; and compliance [79,80,81]. Despite these limitations, use of historical controls is now customary [81].
A deeper examination reveals that GC treatment is just one example of the uncontrolled variables affecting historical databases. These variables can be categorized by their origins: external variables, including SOC such as GCs, assisted ventilation, assisted coughing, and lung volume recruitment [82]; intrinsic variables, including a patient’s pulmonary phenotype, which can make their respiratory course unexpectedly mild or severe; the presence and severity of scoliosis, if applicable; and technical variables, such as the fact that height measurements can become inaccurate when patients lose ambulation, affecting the calculation of their FVC %pred [83].
All these variables affect pulmonary function; their influence can be substantial, and their nature and impact will vary. For example, one individual in the historical control group may have a detrimental pulmonary phenotype; another individual might be non-compliant with GC therapy. The pulmonary function of each of these individuals will be worsened, but the causes differ, as may the severity. Considering these variables, it is unsurprising that databases used as historical controls report wide variability in their annual rate of decline of FVC %pred, as described above.
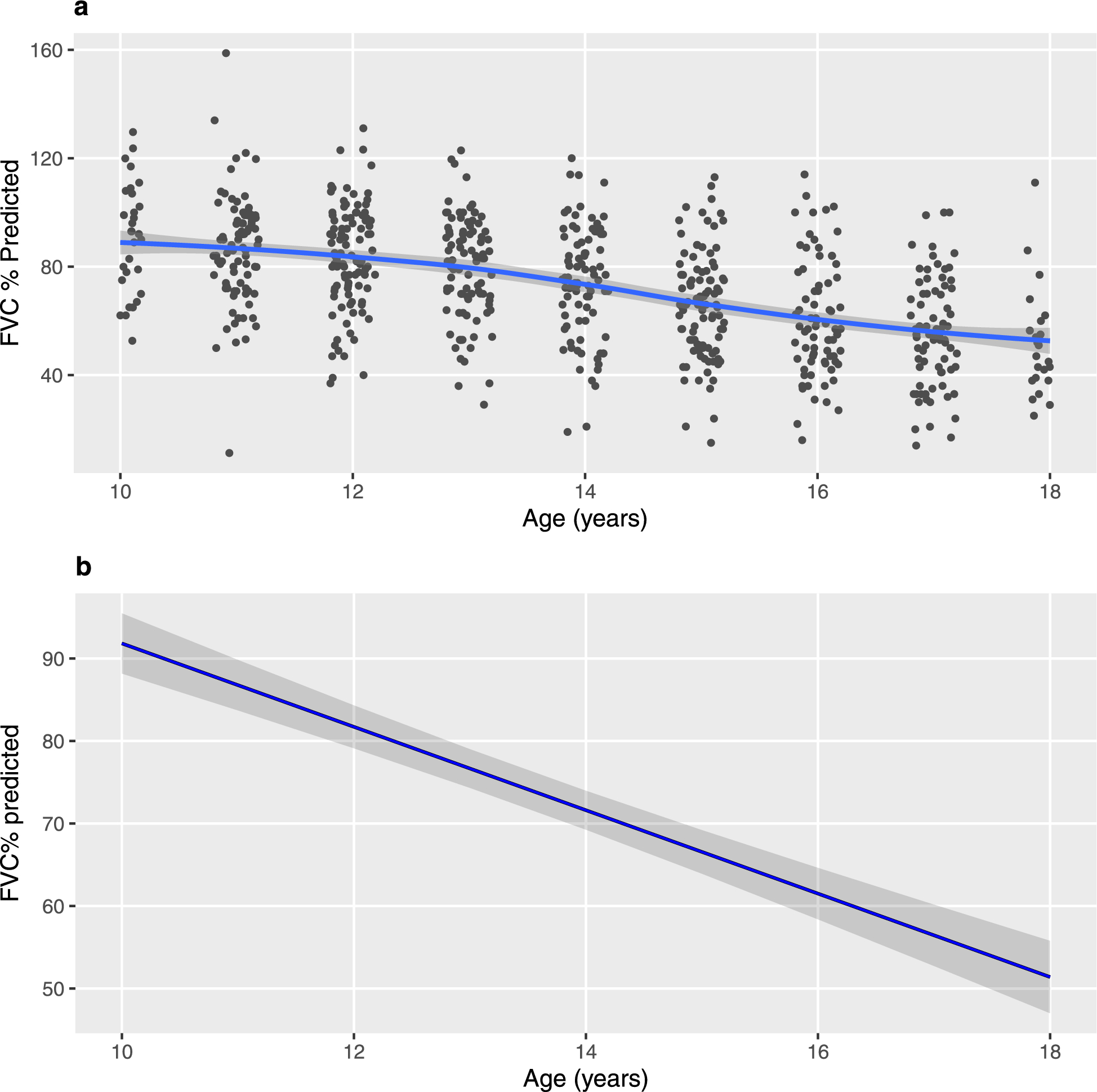
To better understand how historical controls may inaccurately mask pulmonary function variability, we examined data from the CNDR, a large multicenter database of more than 400 patients [84,85,86]. With the support of the CNDR, we re-analyzed their respiratory data and statistically converted individual pulmonary function results into a single annual rate of decline in FVC %pred, as is done by the databases currently used as historical controls. Figure 1a shows the raw data for FVC %pred by age for individuals aged 10–18 years, the age bracket used by control databases, including CINRG. As discussed, there is a high degree of respiratory variability, with a wide span and considerable scatter of the individual values of FVC %pred. Online Resource 1 in the electronic supplementary material shows that changes in FVC %pred are not constant but instead vary widely from year to year within the age bracket. Finally, Fig. 1b shows the same data in the form that is used for controls—a single, constant rate of decline across the entire age bracket. Overall, the statistical analysis employed by historical controls results in a single, constant rate of decline that inaccurately masks the intrinsic variability of the study population (i.e., variability in individual values of FVC %pred and variability in the annual rate of FVC %pred decline). Our analysis illustrates a flaw in existing historical databases, and the findings are not likely due to the unique characteristics of CNDR. Canada has a publicly funded national health system, and individuals with DMD receive care at specialized centers. If anything, this standardized approach to treatment should minimize the effect of uncontrolled variables on pulmonary function [86].
The CNDR data also illustrate how, when historical databases such as CINRG choose the age bracket of 10–18 years as representative of their population, they are choosing the most pessimistic rate of decline [64]. The annual rate of decline of FVC %pred for the overall CNDR population is −3.19% per year. However, the rate of decline for the group aged 10–18 years is −5.1% per year. The same is true for the CINRG database: the age group 10–18 years displays the fastest rate of decline in the whole population [64]. When this pessimistic rate of decline is reported as representative of the overall historical control group, it lowers the bar that the treatment group must attain, making it easier to claim efficacy for a study drug. The fact that this age group is the most pessimistic one supports our prior hypothesis about etiology of the variability. In that age group, a number of key events may occur: GC therapy may be discontinued, negatively impacting pulmonary function; LOA can occur, causing inaccuracies of height measurement and calculation of FVC %pred; and pulmonary phenotypes become divergent, with the potential for individuals to express an unexpectedly mild or severe course of respiratory function. Thus, the annual rate of decline in FVC %pred may be most severe in those aged 10–18 years because that is the age range when the largest number of uncontrolled variables are active, variables that confound the ability of historical control data to isolate and assess the effect of a new drug on pulmonary function.
Despite these concerns, a single rate of decline in FVC %pred is the respiratory outcome measure of choice reported by historical databases [62, 63, 65, 72], and it is almost always used as the control comparator in studies of new drugs. Next, we examine the limitations of FVC %pred as an outcome measure in greater detail.
3.4 FVC % Predicted is a Suboptimal Pulmonary Outcome Measure
In patients with DMD, FVC %pred begins declining in childhood, at or not long after the earliest age that pulmonary function testing can be performed, and the decline continues throughout an individual’s lifespan [64, 87].
Studies of new drugs have adopted FVC %pred, and its annual rate of decline, as their preferred respiratory outcome measure. First, a single rate of decline is determined statistically among individuals spanning an age range (typically 10–18 years); that rate of decline is assumed to remain constant [64, 73]. Those are the historical controls, sourced from one of a few historical databases. Their rate of decline is compared with the rate among subjects treated with a study drug. If the rate of decline in the treated subjects is statistically better than the rate in the historical controls, a beneficial effect on pulmonary function is claimed.
However, the effect of DMD on pulmonary function varies over time and is a product of progressive muscle weakness, the hallmark of the disease. It is therefore inaccurate to apply a single, constant rate of respiratory decline to individuals as they age. For example, the age bracket 10–18 years typically spans the ambulatory to late non-ambulatory stages of the disease, reflecting progressive weakness with aging and heterogeneity of muscle strength.
It is helpful to understand pulmonary function in DMD in the context of unaffected individuals. In a healthy population, lung function rises through puberty, plateaus in early adulthood, and then declines from about 30 years of age [88, 89]. The rate of rise in FVC abs is especially rapid in adolescence, corresponding to linear growth acceleration during puberty (Fig. 2). Overall, in a healthy population, linear growth is the primary driver of the impressive rise in pulmonary f




留言 (0)