
記住我
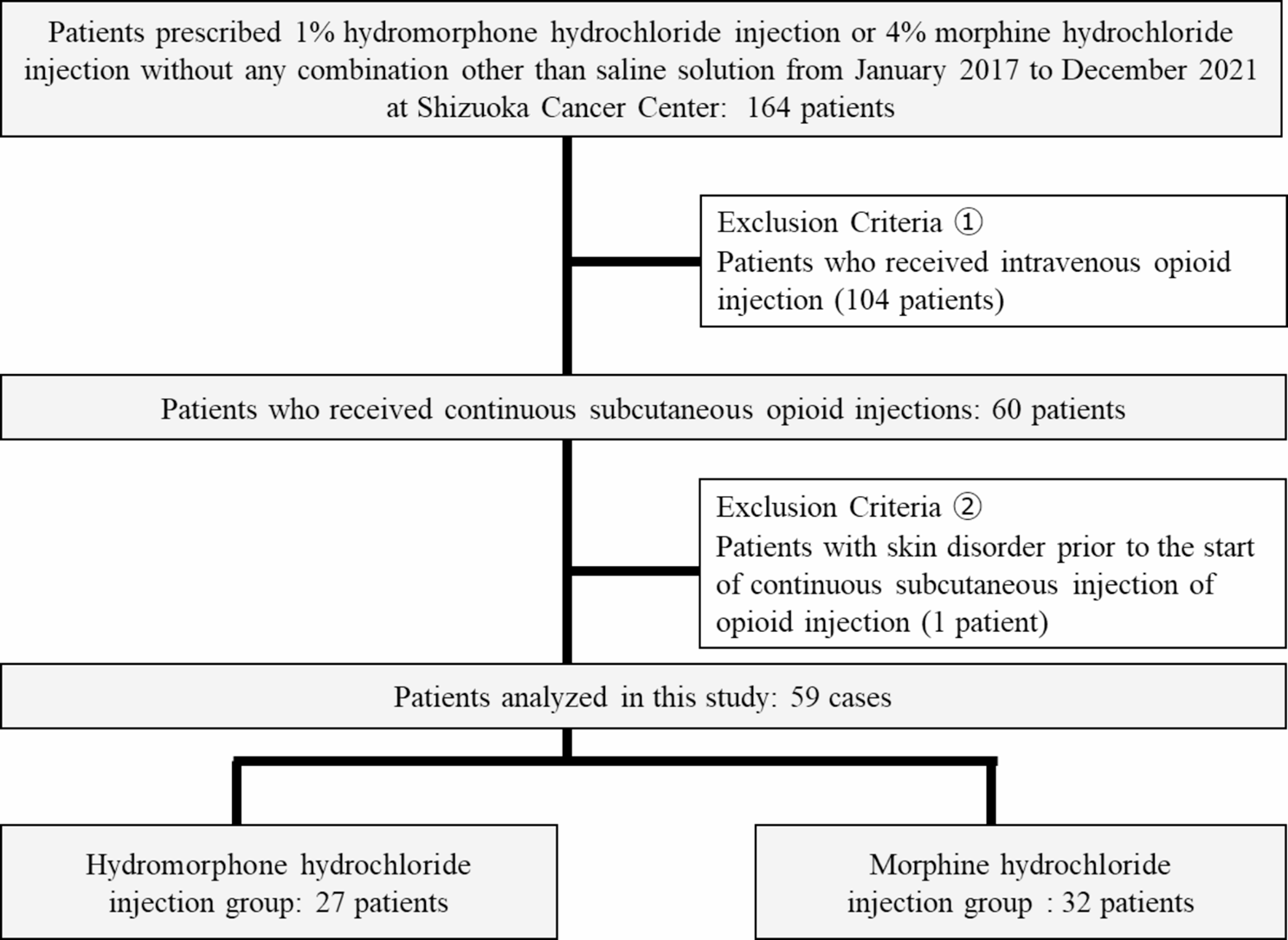


Patients who received continuous subcutaneous administration of 1% hydromorphone hydrochloride and 4% morphine hydrochloride without any combination other than saline for cancer pain at the Shizuoka Cancer Center between January 1, 2017, and December 31, 2021, were defined as participants. The observation period was defined as the period during which 1% hydromorphone hydrochloride and 4% morphine hydrochloride were administered. Patients who received intravenous opioid injections and those who had skin disorders prior to the start of continuous subcutaneous opioid injections were excluded from the study.
Investigation itemsThe primary endpoint was defined as the cumulative incidence of all skin disorders (induration, redness, bleeding spots, burning, and itching) at Gr 1 or higher using Common Terminology Criteria for Adverse Events Ver 5.0 during the entire study period. Age, sex, Eastern Cooperative Oncology Group Performance Status (PS), Body Mass Index (BMI), concomitant medications, starting flow rate, daily dosage (morphine hydrochloride injection equivalent) at the start of treatment, dilution with saline solution, and administration period were investigated retrospectively from the electronic medical record as background factors related to skin disorders. Concomitant medications were defined as steroids (dexamethasone, betamethasone, prednisolone, methylprednisolone, fludroxycortide, and fluticasone propionate), non-opioid analgesics (loxoprofen, diclofenac, naproxen, sulpyrine, flurbiprofen axetil, and acetaminophen), and anti-histamines (famotidine, ranitidine, diphenhydramine, fexofenadine, and bilastine) administered at least once for approximately three days from the start to end.
Statistical analysesThe participants were categorized into hydromorphone hydrochloride and morphine hydrochloride injection groups, and the cumulative skin disorders incidence was compared using Cox proportional hazards model analyses and Fisher’s exact test. In addition, age (< 75 / ≥75 years) [20], sex, PS (≤ 3/ 4), BMI (< 25 / ≥25) [21], concomitant medications, starting flow rate (< 0.5 / ≥0.5 mL/h) [10], daily dosage (< 60 / ≥60 mg/day of morphine hydrochloride injection) [22], dilution with saline solution, and administration period (< 28 / ≥28 days) [18] were compared by Fisher’s exact test. Univariate logistic regression analysis was performed to analyze factors influencing skin disorders, such as hydromorphone hydrochloride injection use (or absence of morphine hydrochloride injection), age, sex, general condition, BMI, concomitant medications, starting flow rate, daily dosage, dilution with saline solution, and administration period between the skin disorders occurrence and non-occurrence groups. In addition, background factors with P < 0.2 were adopted in the multivariate logistic regression analyses [23].
Since concomitant medications have been shown to be a risk factor for subcutaneous injection-derived skin disorders in previous reports [24,25,26,27,28], concomitant steroid use, non-opioid analgesics use, and anti-histamine use were included as factors in the multivariate analysis, even if the P value in the univariate analysis was ≥ 0.2. Chi-squared analyses were conducted for the adopted background factors based on the degrees of freedom and scale ratio to test the significance of the regression analysis. All statistical tests were run in Bell Curve for Excel (Social Survey Research Information Co., Ltd.) at 5% statistical significance level.
Ethical considerationThis study was conducted in compliance with the “Ethical Guidance for a Study in Medicine-Targeted Humans” and was approved by the Institutional Review Board of the Shizuoka Cancer Center (approval number: J2021-174-2023-10-3).
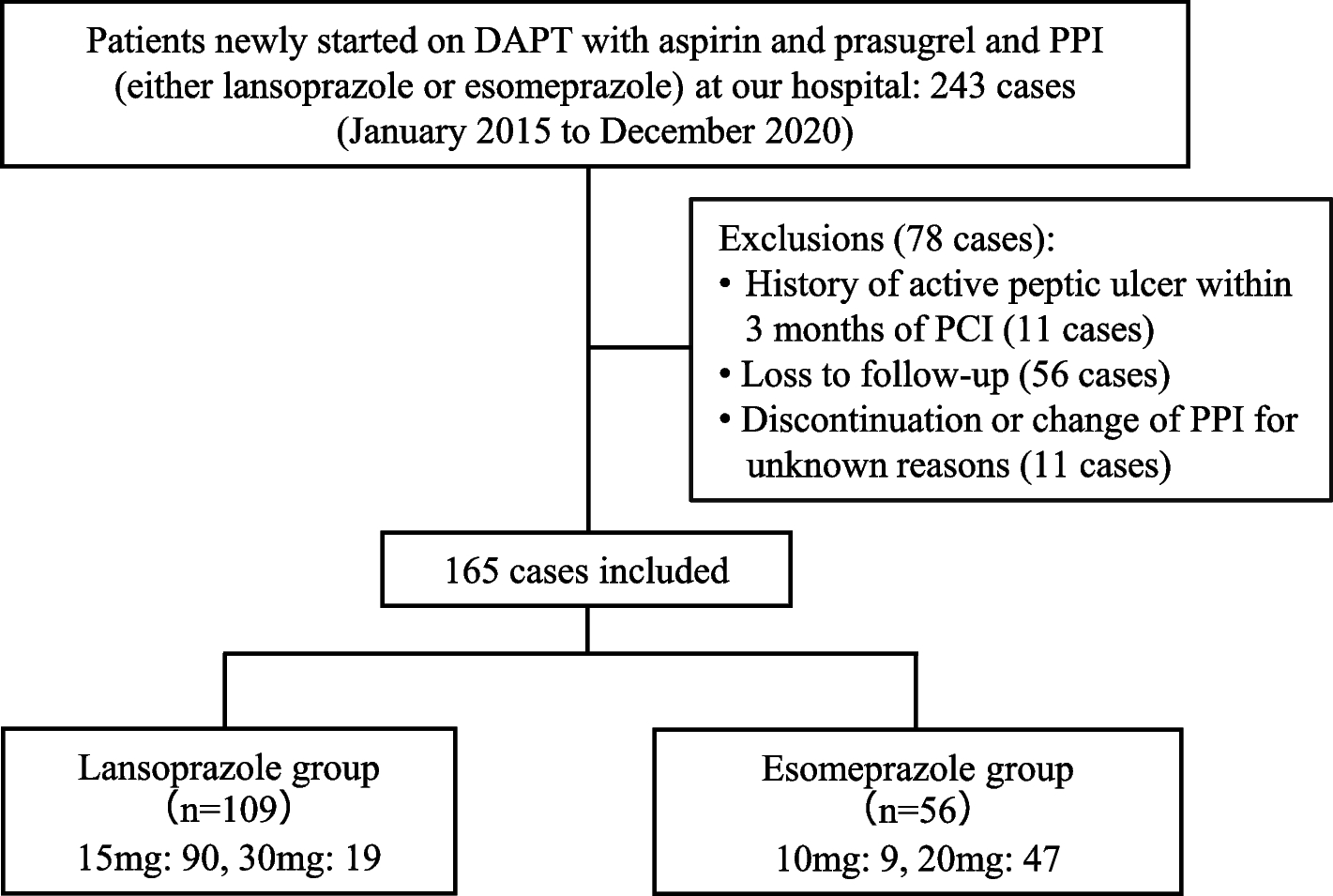
Fig. 1
Flow diagram of patient selection. The number of patients excluded in this study are shown
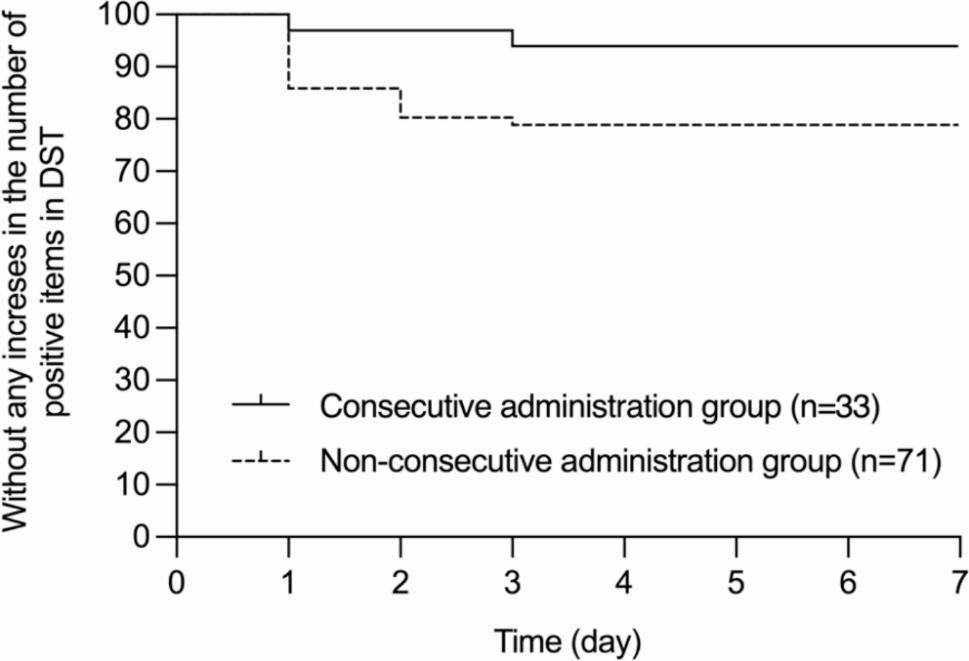
Fig. 2
Comparison of cumulative incidence of skin disorders. The date of onset and incidence of skin disorders are shown in hydromorphone hydrochloride group and morphine hydrochloride group
留言 (0)