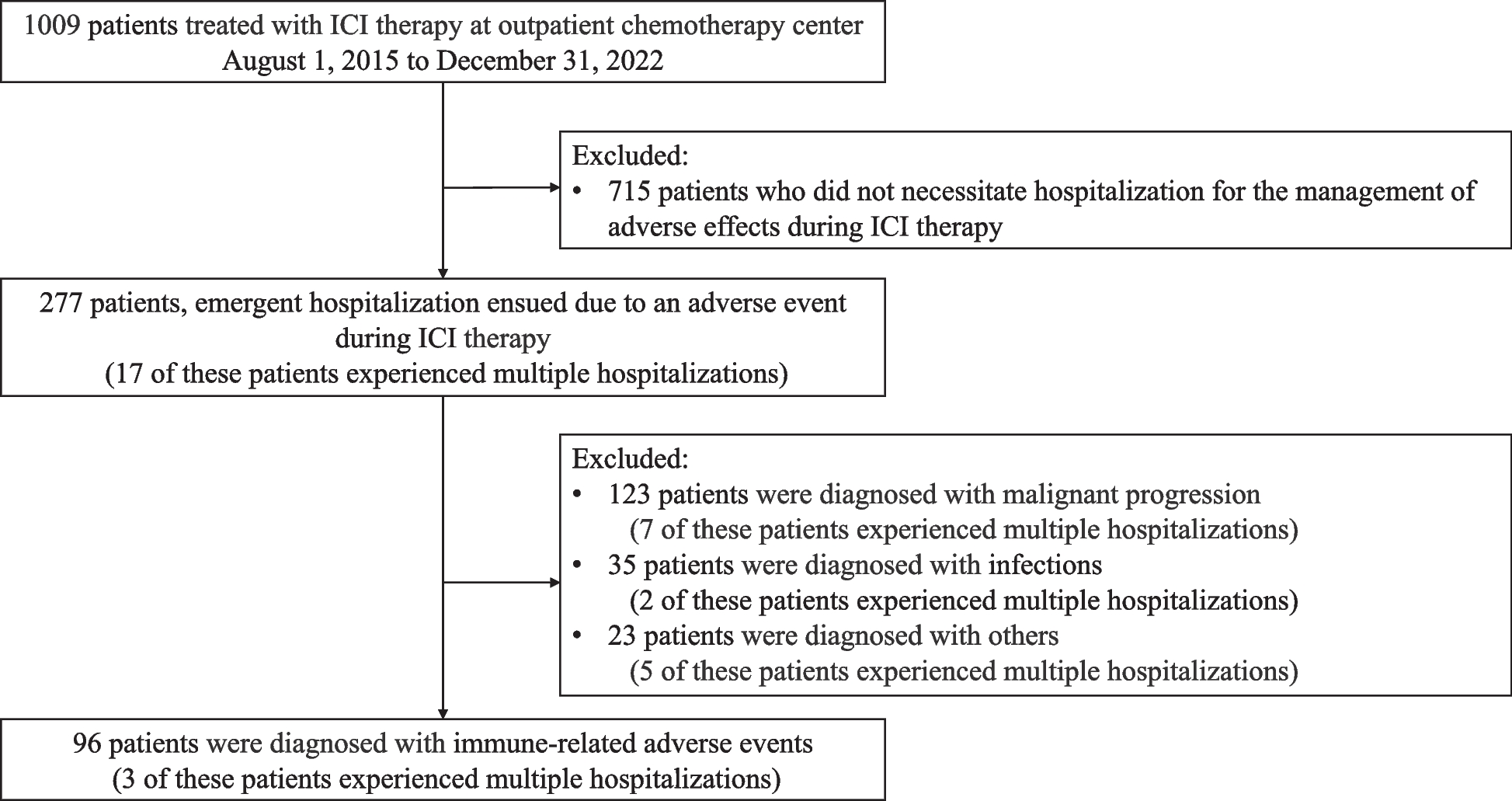
Over the 7-year study period, 1009 patients received ICI therapy at our institution, with 96 patients requiring emergency hospitalization due to irAEs, with a hospitalization rate of 9.5%. Moreover, 47.9% of hospitalized patients required unplanned medical facility visits, highlighting the need for interventions beyond standard clinical protocols. Clinical trials of approved ICIs have reported emergency hospitalizations in fewer than 5% of patients [15,16,17]. In contrast, our study indicated a higher frequency of emergency hospitalizations, suggesting a potentially increased incidence of irAE-related emergencies in real-world settings. These findings underscore the importance of understanding the clinical characteristics of emergency hospitalizations for irAEs and advocating an emergency response framework that ensures continuous monitoring and prompt intervention.
Approximately 40% of the emergency hospitalizations due to irAEs in our study occurred within the first 3 months of treatment, consistent with previous reports showing irAE onset within 2–3 months of ICI administration [18, 19]. Early monitoring of irAE onset and severity is therefore crucial for effective management. In this study, treatment intervals for scheduled hospitalizations ranged from 2, 3, 4, and 6 weeks. While this variation reflects the flexibility of ICI treatment regimens, longer intervals may delay irAE detection and increase the risk of emergency hospitalization, whereas more frequent visits may allow earlier detection and reduce the need for emergency intervention. Thus, patients with long intervals between visits require careful monitoring, including the use of telecommunications. The nearly equal frequency of routine and emergency visits in our study also highlights the limitations of relying solely on routine outpatient visits to manage ICI-related adverse events. Given the unpredictable nature and variable frequencies of irAEs, it is essential to establish a comprehensive management framework. Additionally, raising awareness of irAEs and educating patients, caregivers, and healthcare providers about symptoms that require immediate medical intervention is crucial. The high number of unscheduled visits in our study emphasizes the need for better monitoring and patient education. Structured monitoring programs focused on early detection of irAEs, particularly in the first few months of ICI therapy, can help identify symptoms before they escalate. Telemedicine and regular follow-ups may also reduce emergency visits by providing timely interventions [20,21,22]. Educating patients and caregivers to recognize early symptoms and seek prompt medical attention is essential to prevent unscheduled hospitalizations [23, 24].
Early detection of irAEs requires not only routine testing, but also a comprehensive and timely assessment focused on the patient's chief complaint. In our study, dyspnea was associated with respiratory symptoms and diarrhea with gastrointestinal toxicity. However, symptoms such as fatigue, anorexia, and vomiting did not show a strong association with specific irAEs. This reflects the non-specific nature of these symptoms and their common occurrence with some irAEs. Fatigue and malaise in cancer patients are multifactorial, caused by both malignancy and chemotherapy, with an incidence of over 60% [25, 26] This reflects the complexity of irAE management and suggests that such symptoms should be carefully monitored, and further diagnostic evaluation is needed to determine the cause. The high rate of emergency presentations in this study among patients presenting with fatigue and fever also suggests the need for patient education to encourage early consultation. Although this study focused on irAE, distinguishing irAE from cancer progression or comorbidity remains a challenge in clinical practice. Early recognition and management can significantly improve patient outcomes and reduce the risk of serious adverse events [27].
This study included 96 patients diagnosed with irAEs requiring emergency hospitalization. Of these, 16 patients with endocrine disorders were excluded from the analysis due to differences in treatment compared to other irAEs. Additionally, patients admitted solely for further evaluation or for reasons unrelated to irAE treatment were excluded from the primary analysis. This ensured the focus remained on patients who required emergency hospitalization for irAE treatment. Among the remaining 80 patients, 62 received corticosteroids, the primary treatment for irAEs, although some patients received antibiotics or alternative therapies, and others improved spontaneously. This discrepancy between guideline-recommended treatment and real-world clinical practice is a notable finding of this study. Conversely, eight patients died due to irAEs, underscoring the potential impact of appropriate irAE management on patient prognosis. Although not all irAEs requiring hospitalization are severe, some require immediate intervention, emphasizing the need for rapid escalation protocols in irAE management. In this study, 34.3% of patients requiring emergency hospitalization for irAEs resumed ICI therapy. Although ICI therapy is crucial in cancer treatment, the risk of recurrent or worsening irAEs remains concerning. Previous reports indicate that approximately 30% of patients experience irAE recurrence [28], suggesting that restarting ICI therapy should be carefully weighed against the potential risks and benefits.
This study has inherent limitations. Its retrospective design depended on the accuracy and completeness of medical records, which may have introduced bias. Furthermore, the study was conducted at a single institution, limiting generalizability to broader populations or settings. Although the sample size was substantial, rare irAEs may have been underrepresented. Future studies should aim to incorporate more comprehensive data collection methods, including standardized grading of symptoms and clarification of overlapping clinical presentations, to provide a more detailed understanding of irAEs. Another limitation is the lack of a direct comparison between patients requiring emergency hospitalization due to irAEs and those who experienced irAEs but did not require hospitalization. While this study focuses on patients who required emergency intervention, a broader comparison with non-hospitalized patients could provide additional insights into the overall management of irAEs. Future research should explore this comparison to enhance understanding of the full spectrum of irAE severity and its management during ICI therapy. Finally, the retrospective nature of the study meant that medical records did not consistently document the severity of irAEs, limiting our ability to fully analyze symptom severity. While the Spearman rank correlation identified associations, it did not establish causality, necessitating prospective investigations to confirm and elucidate these relationships.



留言 (0)