Study population
Patients treated intravenously with tobramycin, amikacin (AMK), GM, or arbekacin were included in this study. Patients undergoing renal replacement therapy, those with < 2 days of treatment, and those aged < 18 years were excluded. The study period ranged from January 1, 2014, to December 31, 2023, with the pharmacist-led TDM intervention starting on January 1, 2017. Medical records were retrospectively examined to assess the effects of this intervention.
Ethics approval
This study was approved by the Ethics Committee of our hospital (approval number: 202401). Further, this study was conducted with comprehensive opt-out consent obtained from all participants.
Pharmacist-led intervention
The following pharmacist-led TDM intervention (hereinafter referred to as “the intervention”) was initiated on January 1, 2017. First, pharmacists identified patients with new prescriptions for AGs during the weekday day shift. Second, all newly prescribed patients were charted for the need for AGs and recommendations for appropriate dosage and blood concentration measurements. Third, physicians were contacted by phone if there was no justification for AG use or if dosage deviations occurred. Fourth, follow-up with the patients was performed every weekday during the day shift to determine if AGs were required and if there were any TDM issues; consultation was performed with the physician by phone, chart notes, and the ward pharmacist, as required.
In this study, before the intervention, the pharmacist provided feedback on the simulation results only when blood concentrations were measured at the physician’s discretion. Moreover, a physician’s order to measure blood concentrations was conducted to measure peak and trough concentrations.
Evaluation of outcomes
This study retrospectively compared AG use before and after the intervention. The appropriateness of AG dosing was evaluated based on weight documentation, renal function monitoring, and infection site or pathogen considerations. In this study, adjusted body weight was used to assess AG dose adequacy in patients with ≥ 20% of their ideal body weight (IBW), as follows: IBW = A + 0.91 x [height – 152.4], where A is 50 for men and 49.5 for women; and adjusted body weight (kg) = IBW + [0.4 x (actual body weight - IBW)]. In addition, based on adopted formulation standards and clinical practices, appropriate dose tolerances were less than ± 100 mg for AMK and less than ± 60 mg for GM, tobramycin, and arbekacin (Additional File 1, Table S1). When the minimum inhibitory concentration of the causative organism was unknown, the dose was considered appropriate if within the range based on the patient’s renal function (Additional File 1, Table S1). AG blood concentrations were considered adequate when both peak and trough concentrations were within the recommended range. When only one of these concentrations was measured due to an error during collection, it was excluded from adequacy determination in this study.
AG usage was categorized into three levels: “Recommended,” “Optional,” and “Not recommended,” based on existing guidelines [1, 2, 15,16,17,18], including the Sanford Guide for the Treatment of Infectious Diseases, the guidelines for infective endocarditis, and the guidelines generally used in Japan (Additional File 1, Table S2). The duration of AG use was determined by referring to various medical practice guidelines.
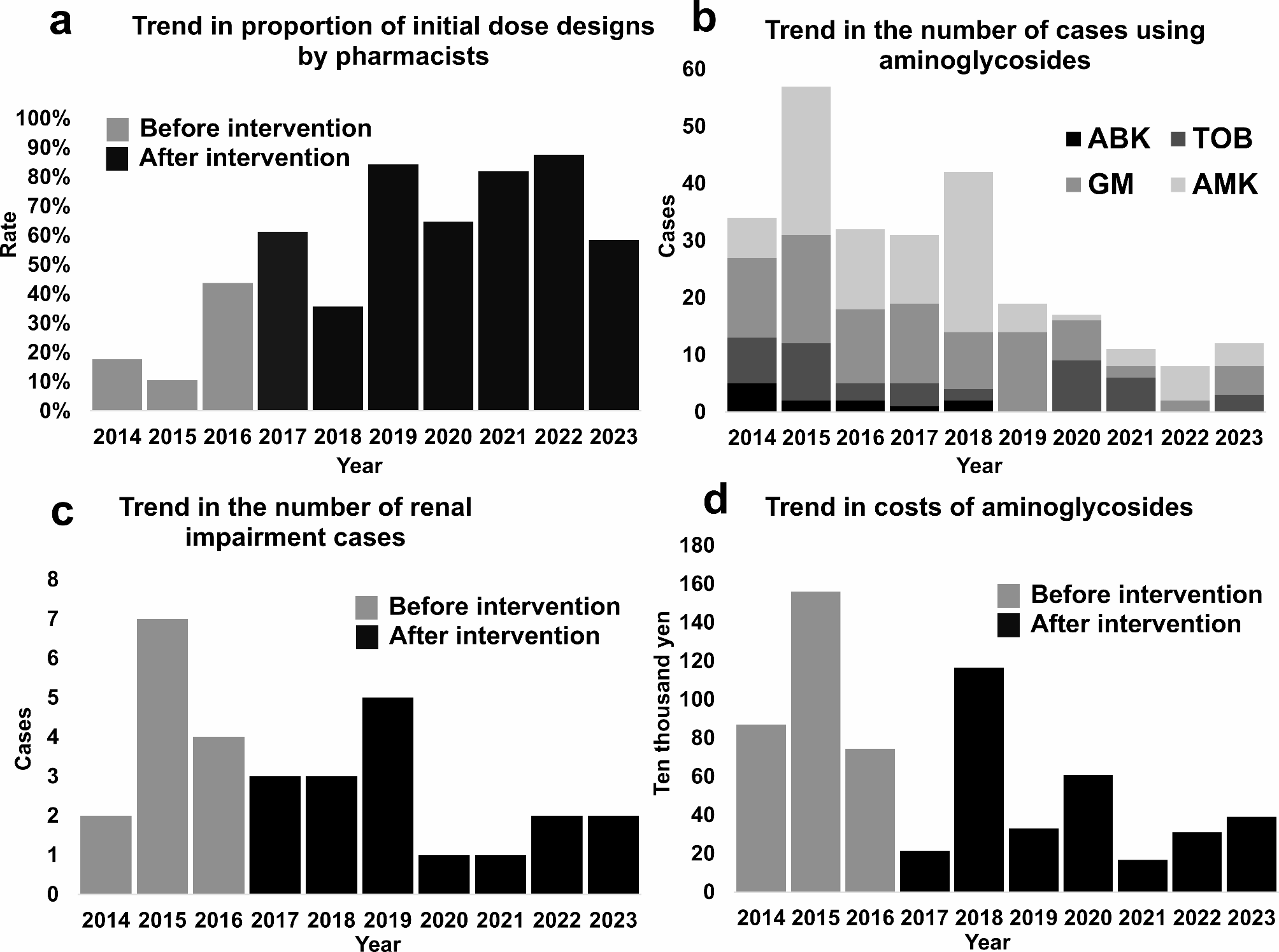
The proportion of first-dose designs by pharmacists, the number of patients using AGs, the number of incidents of renal impairment, and the cost of AG use were also evaluated over time. Renal impairment was defined as a serum creatinine concentration increase of > 0.3 mg/dL or > 1.5-fold before and after AG administration [19] (Additional file 1, Table S3). The cost of AGs used was based on the drug prices as of 2023. Therefore, based on the formulation standards adopted by the hospital, the price per ampule was calculated as follows: tobramycin (60 mg), 403 yen; gentamicin (60 mg), 307 yen; amikacin (100 mg), 350 yen; and arbekacin (200 mg), 5750 yen. Any fractions were calculated as if one ampule had been used.
As a preliminary study, we interviewed five pharmacists routinely involved in AG dosing design and asked how much time was needed to determine AG dosing per patient.
Statistical analyses
Binary variables were evaluated using Fisher’s exact probability test, and continuous variables were evaluated using the Mann–Whitney U test, both with a significance level of < 5%. EZR version 1.68 (Saitama Medical, Jichi Medical University, Saitama, Japan) was used for all analyses [20]. For missing data, statistical tests were performed by substituting the mean value of the item.
As a preliminary investigation, a factors analysis was performed in patients whose AG blood concentrations were determined to be completely manageable without dose adjustments. Logistic regression analysis assessed the factors that allowed for complete control of AG blood concentrations without dose adjustments. Factors included BMI, eGFR at the start of AG dosing, initial AG dose, and type of AG. Receiver operating curves were then drawn for significant factors and cut-off values based on Youden index were calculated.



留言 (0)